Article Text

Abstract
On 29 March 1744, Thomasin Grace, a 13-year-old girl, was the first inpatient admitted to the Northampton General Infirmary (later the Northampton General Hospital). Inpatient hospital diets, then and now, are mainstays of effective patient treatment. In the mid-18th century there were four prescribed diets at Northampton: ‘full’, ‘milk’, ‘dry’ and ‘low’. Previous opinions concerning these four diets were unfavourable, but had not been based upon an individual dietetic assessment. Thomasin would most likely have been given the milk diet, but use of the full diet cannot be excluded.
‘Grace Everyman’ is Thomasin's modern equivalent. Under current NHS guidelines Thomasin would be considered a paediatric patient, but in 1744 she would have been considered as an adult. This study undertakes a full dietetic analysis of all the prescribed diets available for Thomasin in 1744 and compares this against random choices for Grace from the 2009 inpatient menu from the paediatric (Paddington) ward, and the adult ward inpatient menu at the Northampton General Hospital. The results show that, for Thomasin, the 1744 milk and full diets met the current advised nutritional requirements for adequate dietary intake. However, for Grace, the present 2009 Paddington and adult ward menu, although generally meeting nutritional requirements, could, if Grace or her carer consistently chose poorly during a prolonged inpatient stay, lead to inadequate nutrition. This challenges assumptions that hospital diets were historically inadequate, and that choice in present day equates with satisfactory nutritional intake.
- History of medical
- modern medicine
- social history
- child health
- nutrition and metabolism
Statistics from Altmetric.com
Introduction
The Northampton General Hospital is one of the earliest English voluntary hospitals. Its first inpatient on 29 March 1744 was Thomasin Grace a 13-year-old girl (figure 1).

Thomasin Grace's admission entry 1744 (reproduced with permission from the Northampton General Hospital Archive).
Thomasin Grace was an inpatient for 14 weeks and 2 days before she was discharged cured on 7 July 1744. Her condition, scald head, is now recognised to be chronic ringworm, exacerbated by chronic malnutrition.1 In the 18th century, Thomasin would have been classified as an adult patient because she was over the age of 12.2
‘Grace Everyman’ is Thomasin's modern equivalent.3 Today, Grace would be classified as a child and admitted to Paddington ward, one of two paediatric wards at the Northampton General Hospital. Paddington is a general paediatric, non-surgical ward with 27 beds and a three-bed High Dependency Unit. It caters for children from infancy up to 16 years of age. In sharp contrast to Thomasin, Grace's admission would have been far shorter, probably little more than 24 h. For the calendar year 2008, the mean length of stay on Paddington Ward was 1.02 days for the 3380 admissions recorded.
Hospital diets in the 18th century
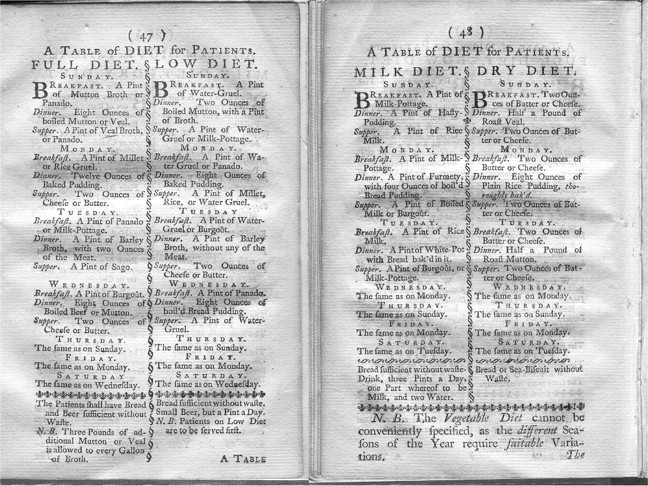
Hospital diets in the 18th century are an under-researched area. In 1744, there were four prescribed diets available: full, low, milk and dry. The regulations of the infirmary did not make a distinction between adults and younger patients (though the general admission of children under 7 years of age was prohibited).4 The Infirmary took great care to ensure that the food dispensed was of generous and good quantity, and well regulated, if somewhat monotonous.5There was some seasonable variability regarding vegetables. A copy of the 1744 menu containing the different ‘milk’, ‘dry’, ‘full’ and ‘low’ diets for patients has survived (figure 2).4

Inpatient menu, Northampton General Infirmary, 1744.
Hospital diets in the 21st century
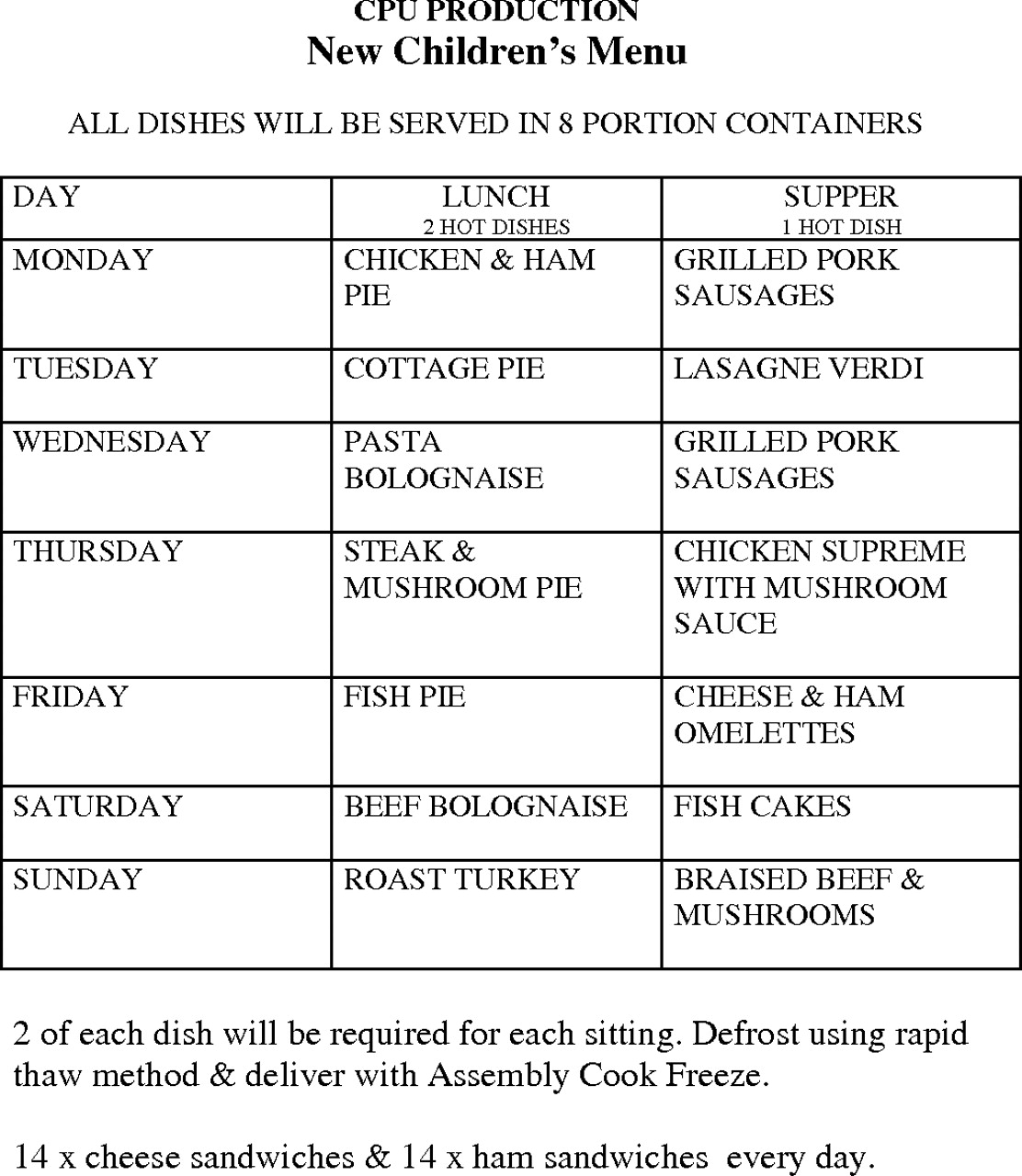
In 2001, the Department of Health published recommendations under the Better Hospital Food initiative.6 All hospitals must provide the estimated average requirement for energy and the reference nutrient intake (RNI) for all other nutrients. For children, the menus should provide the RNI for all nutrients and provide a range of dishes that will be popular and likely to be eaten (figure 3).

{kind=link}
{kind=link}
{kind=link}
Paediatric inpatient menu, Northampton General Hospital, 2009.
Modern diets show greater variety to cater for dietary susceptibilities (such as coeliac disease), religious prohibitions and vegetarianism. Also, special diets are strongly advocated for conditions such as severe epilepsy.7 In 2009, the National Patient Safety Agency assessed the quality of the food provided at Northampton General Hospital as being ‘excellent’.8
Methods
For the purposes of this study, three random menus for adults and three for children were randomly chosen by way of raffle. The adult menus were separated by three different weeks according to the hospital menu. The full details concerning the adult and paediatric menus are given in the supplementary material.
Information about weights of the different selections from the menus was obtained and then assessed in the software dietary analysis programme Dietplan6 (Forestfield Software, Horsham, UK). Some recipes were accessed for the 18th century diets to study exact ingredients, such as hasty puddings and potage. This enhanced the accuracy of the analysis by stating exact ingredients, but not always quantities, for example, recipes stating ‘as much sugar as you shall think fit’. Some exact portion sizes were stated in the menu, including 2 ounces of cheese, 8 ounces of boiled mutton and veal.
However, as with all dietary analysis, there are some inaccuracies where estimates have to be made. This is the case with vegetables where the availability, quantity and cooking time would affect vitamin C intake quite significantly.
Results
The salient results are given in table 1. The full dietetic analysis for all diets are downloadable from the journal website.
Comparison of the 1744 diets with random choices of the 2009 paediatric (Paddington) and adult ward diets adjusted for a 13-year-old girl
Generally, the 1744 milk and full diets have higher energy content than the 2009 diets. The other most striking difference between Thomasin's and Grace's diets is in the amount of choice and the consequence of exercising this. Grace, unlike her 18th century counterpart, has a daily choice of fresh vegetables and, on most days, fresh fruit. Depending upon her selection, Grace can obtain a more varied diet including vegetables, fruit, fibre rich food and fish.
On the adult menu there are 12 different choices of main meal for lunch and 11 for supper, and 8 different choices of dessert for lunch and supper. On the paediatric ward, the children have fewer choices. Except for the main meal, they can choose tuna fish salad and between four vegetarian dishes. Grace's individual choice can lead to great variations in energy and nutrient intake. One example being, were Grace to have randomly chosen the vegetarian sausage instead of the pork sausage, the daily energy content would have been 1668 kcal instead of 2197 kcal.
Grace's average energy content was lower than Thomasin's full and milk diets. However, with Grace's length of stay being so much shorter than Thomasin's, a poor choice within a ward setting would minimally exacerbate an already present nutritional deficiency rather than lead to its development in itself.
Discussion
This is the first attempt to undertake a formal dietetic analysis on published 18th century voluntary hospital menus for a named 18th century patient and compare them with present-day diets. Recent research into child nutrition has concentrated on the diets given from the 19th century onwards;9 18th century English voluntary hospital diets are not an area covered in depth or indeed, where the topic is covered, just adults have been considered.10 11 Rabenn, in 1954, stated that these diets were ‘nutritionally poor and often unpalatable’, but gradually improved throughout the 18th century. However, Rabenn did not offer or cite a dietetic assessment to support this view and, furthermore, the Northampton menus, although very similar to those in his paper, are not cited.12
The dietetic analysis of the 1744 Northampton General Infirmary inpatient menus disagree with Rabenn's opinion. They clearly show that Thomasin would have received an adequate dietary intake depending on the type of diet prescribed. Although the proportions of fat, carbohydrate and protein were different, the 18th century milk and full diets had above recommended requirements in vitamin B12 (>1000%) and zinc (>200%). The main discrepancy would be in vitamin C, as orange juice is routinely available in the present day. The 18th century diet was rich in vegetables, but the degree of boiling would have determined the extent of remaining vitamin C. The wide difference between Grace's choice of either a vegetarian or pork sausage has already been mentioned. It should be noted that, although there is no accommodation for this in the 1744 Northampton menu available to Thomasin, the 1756 statues of the London Hospital do allow dietary accommodation for religious sensibilities, in this case patients who are Jewish.12
Of course one unknowable limitation in this study is that Thomasin would most likely have been far shorter than Grace. Stature is only one of several biological markers of nutritional status.13 In British context, Floud and Harris demonstrated that the mean height for an adolescent born in the late 1950s was more than 11.42 inches taller than adolescents born in the mid-18th century (with a sustained increase in average male heights from 1850 onwards.14 15) It is therefore likely that the energy requirements used in the analysis would be an overestimation for an 18th century child with a smaller body mass.16
In the 18th century, the type of diet used was part of the recommended treatment in which doctors sought to treat signs and symptoms rather than particular diseases.12 This practical concept dates from the ancient regimen attributed to Hippocrates, where diet is recognised ‘to the sick as a powerful aid to recovery, and to the healthy a means of preserving health’.17 However, there was a general consensus with some flexibility within this interpretation and, thus, as Thomasin has no other contemporary medical records, one can only speculate as to which diet was given.18 If Thomasin had been considered a child, she would have been given the milk diet. The Northampton General Hospital Archive holds a copy of John Arbuthnot's An Essay concerning the nature of aliment and the choice of them (1731), one of many tracts that states that ‘Milk is fittest for young Children, tender Flesh Meat for them that are growing, and liquid Meats for such as have acute diseases’.19 Indeed, later medical literature (Pereira, 1843) encourages us to believe that it was likely the milk diet that supported Thomasin's recovery, affording ‘support to the system with least possible stimulus or excitement’.20 Pereira relates ‘It is a good diet for many of the diseases of children, especially those of a “strumous or scrofulous nature”’ (it is perhaps worth noting that milk was a leading cause of TB in this period, and unsterilised supplies remained a danger until the first decades of the 20th century).21 22
If, however, Thomasin would already have been seen as an adult, the full diet would likely have been prescribed and used to ‘restore and support the powers of the system’.20
The patient's experience of the hospital and the diet
We still have an incomplete understanding of the diets of the poor in the 18th and 19th centuries.23 Thomasin's prescribed Northampton General Infirmary diet would appear to be more substantial than that which the local poor could ordinarily afford. The evidence for this is largely anecdotal, but infirmary regulations make the consumption of hospital food by visitors a disciplinary offence.
Of course, what is prescribed is not necessarily what is consumed. Complaints then and now concerning hospital diet were common12 and remain a major concern. Dietary restriction was used by other hospitals as a disciplinary measure. In May 1754, the governors of the Newcastle Infirmary judged a complaint about the meat and beer to be unfounded, leading to the guilty patients being severely reprimanded and ordered to have toast and water for 1 week.24
Thomasin's experience of diet of course is beyond the preparation and content of the food itself. Thomasin's diet itself is far more prescriptive than Grace's. Grace would have had the opportunity to select more, as well as ‘extras’, some of which her family would bring in for her. We cannot know whether this would also have been true for Thomasin. However, in later hospitals, such as was the case in Birmingham in the 19th century, family members regularly brought food, but this was often done secretly and searches were therefore arranged at the entrances to wards.25
Lastly, there is the issue of Thomasin's individual taste. Thomasin may, like many children, have chosen not to eat what was given; even the poorest people are discerning and have their own food preferences. Thomasin herself, especially as hospital stay in the 18th century was measured in weeks, may have come to increasingly resent the control upon her life that these diets represented. It needs to be borne in mind how Thomasin could have been oppressed within the hospital environment. The infirmary regulations emphasised that it admitted only the ‘deserving poor', unable to afford healthcare, and a signed letter of recommendation from a hospital subscriber or Governor was required to ensure admission. After treatment, and on discharge, Thomasin and her guardians were required to express their gratitude to the hospital Governors. Thomasin's inpatient experience in the 18th century would have been very different from Grace's more secular, multicultural, child-friendly environment (all forms of games were prohibited in 1744). In the early 21st century, Grace and her family now work in ‘partnership' with healthcare professionals. Grace would experience increasing patient empowerment with (often unrealistically) high expectations.
The relevance of the past to present practice can have a contemporary flavour with ongoing concerns about hospital diets and their efficacy in promoting patient health and healing. Indeed, a recent editorial in the BMJ emphasised that malnutrition in patients leaving hospital is a significant and increasing health problem, being largely undiagnosed.26 Also, recent findings that patients who have been given fresh locally sourced foods recover at a faster rate than those given the more ‘traditional’ 21st century fare are important lessons to society and health service funding bodies.27 With Grace's admission being almost certainly far shorter than Thomasin's, the issue of chronic undernutrition through hospital food is not going to be an issue. Also, the whole issue about providing choice is to cover the vast range of ages, clinical conditions and associated requirements (eg, an adolescent cystic fibrosis patient with a chest infection will need up to 1.5 times the calorie intake of someone of similar age).28 Another example would be that it is good to have healthy choices for paediatric patients newly diagnosed as being diabetic to encourage healthy eating from the outset (thus, in this context, choice is offered but with guidance about appropriate choices). Therefore there is little cause to call for changes in hospital diets individually tailored to each patient's body mass index (BMI). Ideally, patients should only be offered ‘healthy choices’, however, given the remit of choice it is not possible to guarantee this in all cases.
Lastly, any 13-year-old child presenting today with chronic ringworm exacerbated by malnutrition would hopefully be considered a child protection issue. Although child maltreatment is by no means a recent phenomenon and was known in the 18th century, the state organs to identify and address it at that time were embryonic. Indeed, ‘before the 19th century, the idea that the state should intervene in relationships between parents and their children was almost unthinkable’.29 In the present day, child maltreatment is still an ongoing area of significant government and other healthcare/social professional concern.30–32 Paddington Ward would, therefore, be a place of safety for Grace until all the necessary enquiries were completed.
Thus, in conclusion, the most likely prescribed diets for Thomasin, namely the milk or full diets, were nutritionally adequate, and would have supported her recovery. Grace's 21st century hospital diet for the paediatric and adult wards, on the other hand, allows a wide range of nutritional outcomes, dependent on whether she chose well or badly.
Acknowledgments
We would like to thank Mr Bob Butcher and Mr David Moscrop for providing the present day admission discharge data, the Richmond Medical Library, William Kerr Building, Northampton General Hospital, and the History of Medicine Unit, University of Birmingham for their support and Dr Margaret Holloway for her comments. Mrs Noreen Clydesdale and Dr Win Zaw for creating components of the supplementary material. Grace Everyman is a fictional patient and is not inspired by any patient of that name personally known to us living, or dead.
Footnotes
Competing interests None.
Patient consent Dr Andrew Williams is the curator of the archive at Northampton General Hospital and gave consent to use material from the archive.
Provenance and peer review Not commissioned; not externally peer reviewed.