Article Text

Statistics from Altmetric.com
Background
The implementation of the Affordable Care Act (ACA) has spurred a renewed focus on the concept of value, or health outcome per cost expended.1 Though interventions have generally centred around insurance reform and healthcare delivery, medical technology comprises a significant component of US healthcare costs and is an underemphasised sector in the push for reform. The drivers of medical technology costs, accounting for as much as 65% of the increase in overall healthcare spending, include developing new or improved medical procedures, pharmaceutical products and devices or diagnostics.2
Currently, medical technology development and sales are concentrated in high income countries (HICs). In 2009, approximately 75% of the sales of medical devices were in the USA, Japan and Europe.3 Currently, only 13% of manufacturers are located in low and middle income countries (LMICs). Despite this asymmetric market, there is both growing interest and market potential in investing in health technologies in LMICs, as evidenced by a recent WHO report analysing medical devices in LMICs.4 Nine of the top 10 medical device companies state in their annual report that they hope to expand their activities in emerging markets.5 In Africa alone, there has been a 7.5% annual increase in the importation of medical devices.6
With a new emphasis on value in the US healthcare sector, and an increased interest globally in the development of medical technologies, investing in low cost health technologies could be of mutual benefit to both high and low income countries.4 In addition to filling a great need in LMICs, ideas can flow from LMICs to more developed countries in a process called Reverse Innovation.7
Traditional medical technology innovation arises in academic medical centres, pharmaceutical companies or biotechnology companies in HICs. In the traditional model, products were stripped down or donated to LMICs.8 This model of innovation failed to take into account the qualities of LMICs that serve as advantages to driving out-of-the-box solutions. These qualities include: unique preferences that inspire creativity, overwhelming need, room in the physical and social infrastructure for rapid implementation of novel technologies, and social and economic incentive for Value-Based Design. In this article, we build on the concept of Reverse Innovation with Value-Based Design and Co-creation, and describe how the Consortium for Affordable Medical Technology (CAMTech) incorporates these principles to create low cost medical technologies for LMICs.
Discussion
Reverse innovation and Value-Based Design
Reverse Innovation, defined as the flow of ideas from low to high income settings, has gained traction in the business world, and only recently has been applied to the healthcare setting. The potential for Reverse Innovation in Healthcare is great; in a literature review, Syed et al9 find that the benefits of Reverse Innovation span all six WHO building blocks of health systems. In a recent article by Lord Nigel Crisp, the public health expert calls for further development and implementation of the Reverse Innovation concept.10 The model for Reverse Innovation in healthcare developed by DePasse and Lee,11 shown in figure 1, describes four steps in the Reverse Innovation pathway. Step 1 involves identifying a problem common to low income and high income countries. Step 2 is low income country innovation and spread. Step 3 is cross over and step 4 is HIC innovation and spread.
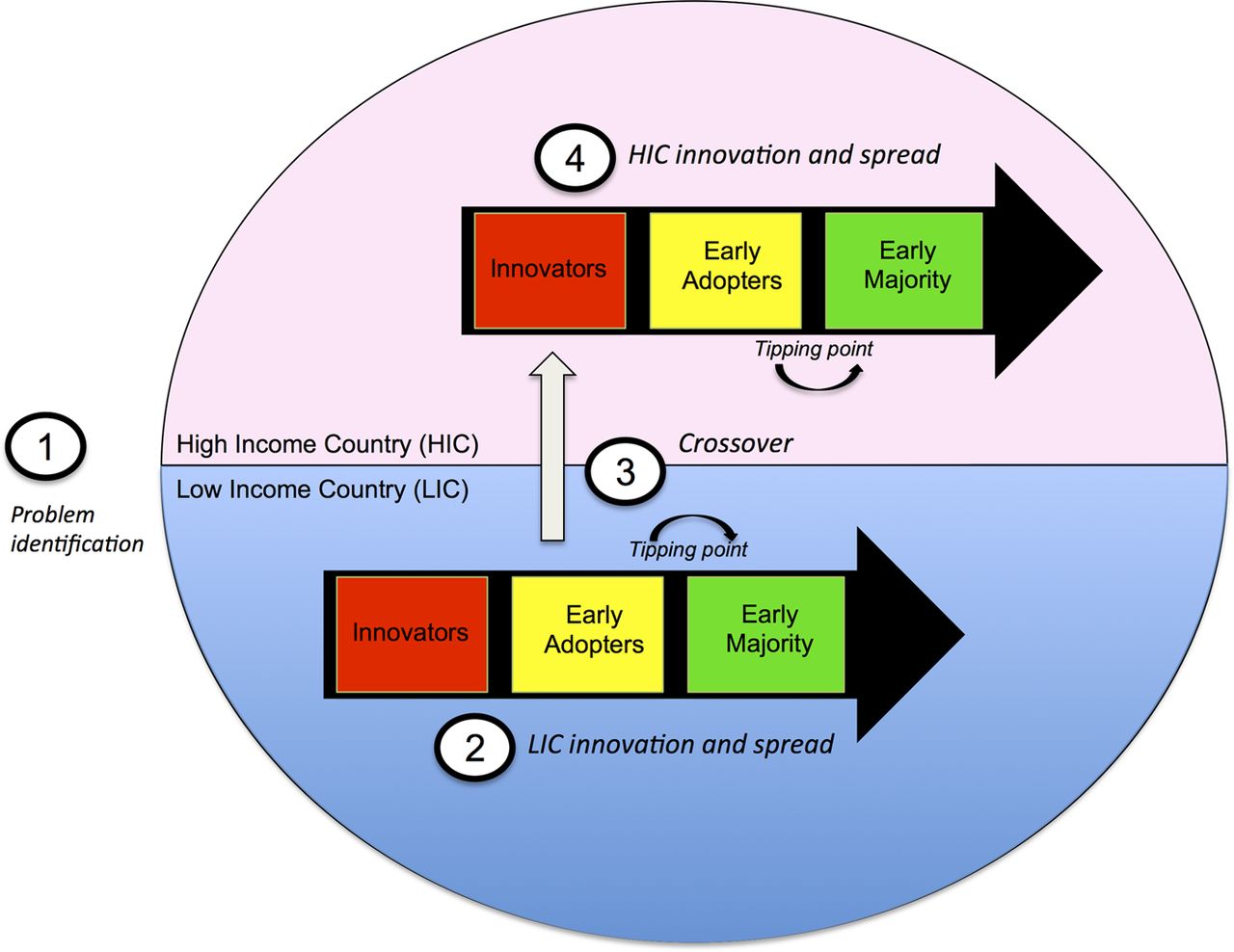
A model for Reverse Innovation in healthcare. Adapted from DePasse and Lee.11
Step 2, promoting entrepreneurship in low income settings, is a historically neglected area. Little investment has been made that is specifically aimed at technology development and commercialisation in resource-poor areas. In addition, traditional forces in developed world markets have not incentivised Value-Based Design for medical technology.
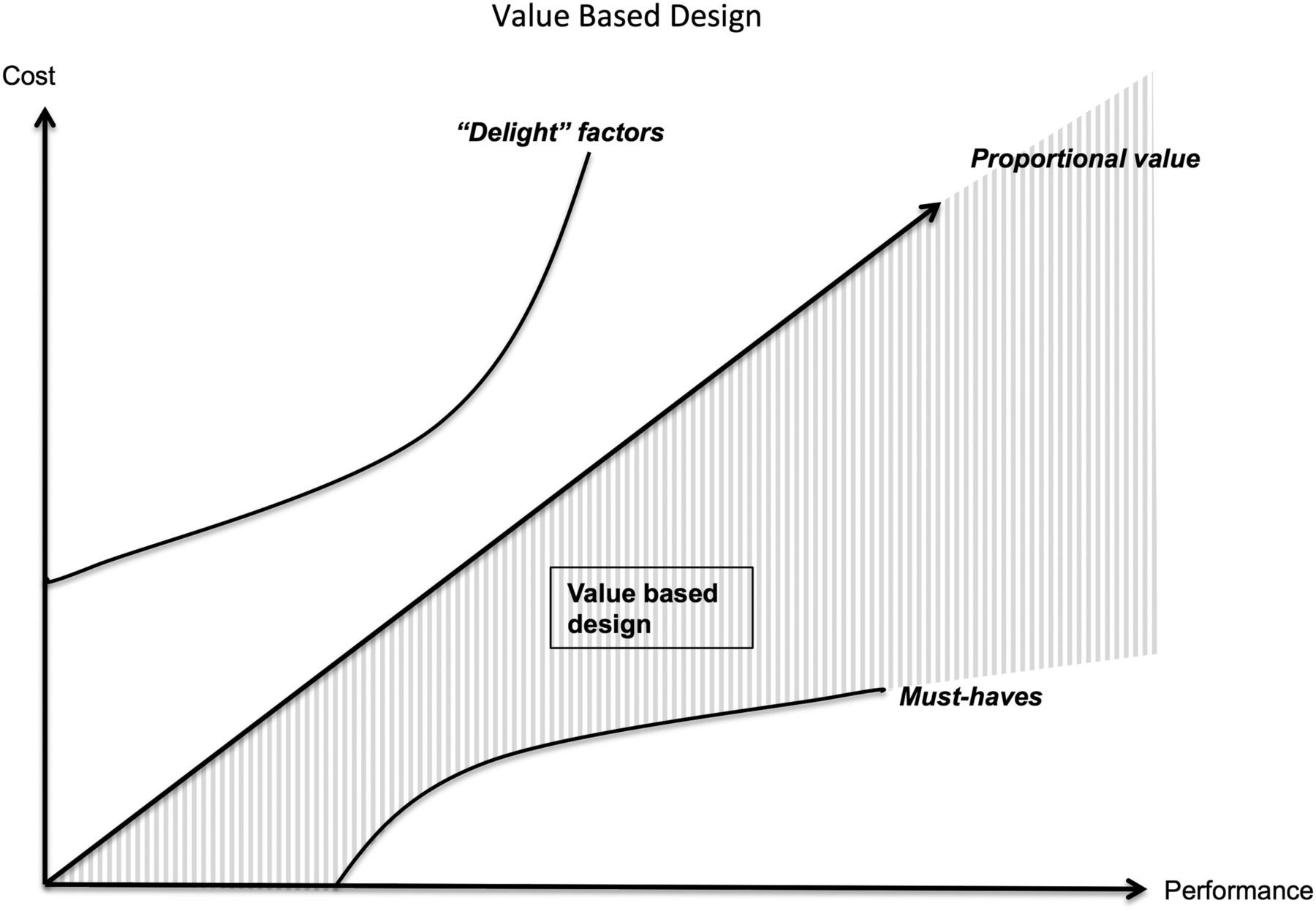
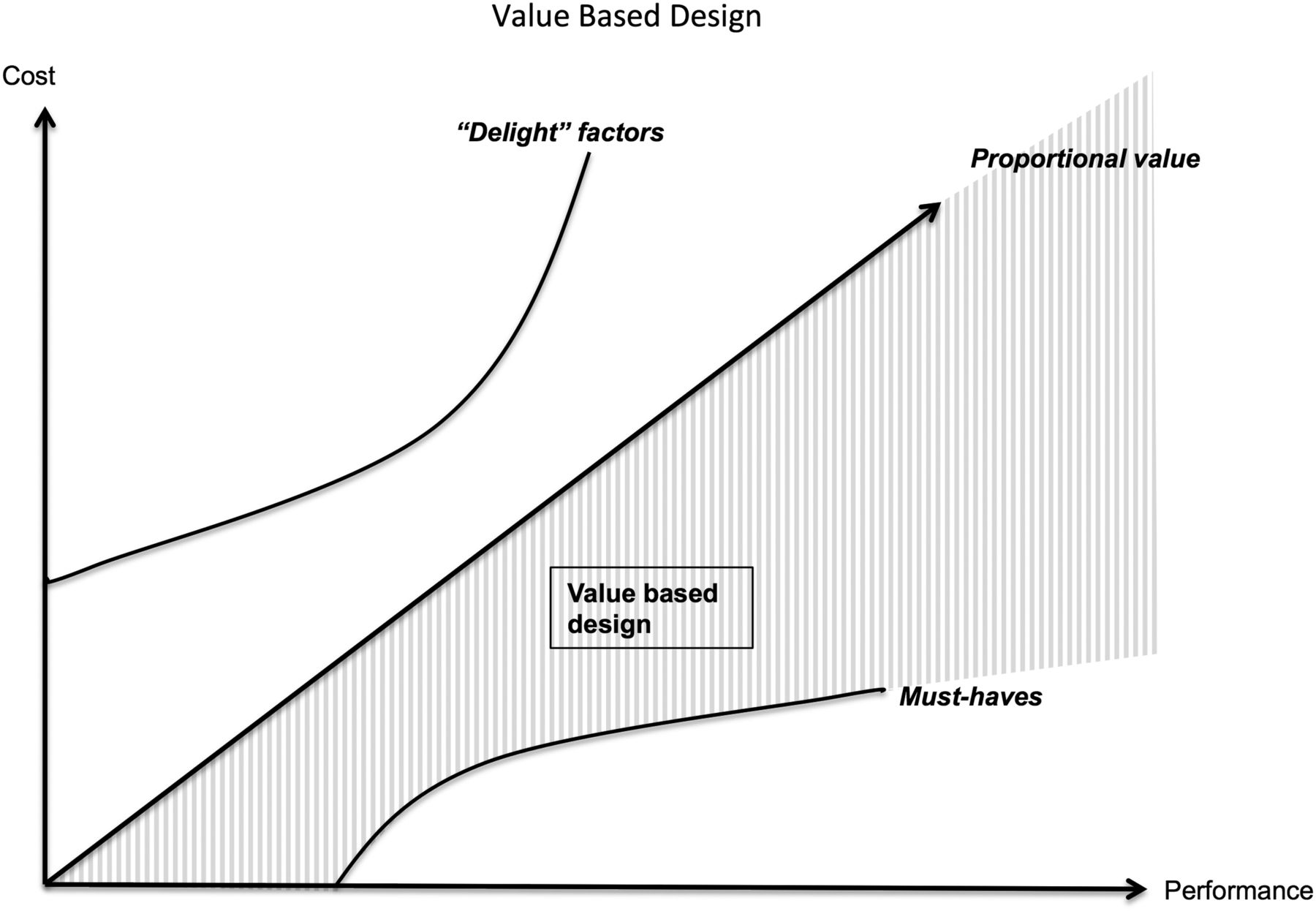
Figure 2 represents a model of Value-Based Design, using an adaptation of the Kano business model,12 in which the x-axis represents performance, and the y-axis represents cost. Traditional healthcare market forces in developed countries incentivise extra ‘delight’ features, or costly technological features that do not impart proportional performance increases. For example, recently, costly imaging modalities such as MRI were used in the screening of breast cancer, though studies have now shown that this method is only effective in a very narrow subset of patients.13 Pharmaceutical companies have developed enantiomers of their compounds to re-patent and sell as superior to the generic choice, though no clinical evidence may exist suggesting improved performance.14 New neonatal incubator models often are sold with added-feature such as X-ray trays, though studies have shown that they may be rarely used or superior in practice.15 These features provide marginal utility at an exponential cost.
{kind=link}
{kind=link}
Value-Based Design. Based on the Kano business model.
The addition of ‘delight’ features has traditionally helped biotechnology and pharmaceutical companies increase profitability, though often without proportional increases in performance. However, recognising that healthcare is an imperfect market, Value-Based Design moves away from this traditional model and instead optimises the performance-to-cost ratio. The lower theoretical limit of enhancing value would be to maintain features above a minimum ‘must-have’ threshold for devices while increasing the performance-to-cost ratio. By focusing on Value-Based Design, we can incentivise entrepreneurship in LMICs and HICs.
Co-Creation model to enhance Value-Based Design
We build on Reverse Innovation and Value-Based Design models with a process called Co-Creation. Co-Creation recognises the need for cross-disciplinary and intergeographic teams to work in concert throughout the product development pathway.16 Co-Creation facilitates the development of innovative medical technologies by employing iterative contributions from individuals in engineering, health and business in LMICs and HICs. In addition, end-users—both providers and patients—are included longitudinally in the development teams. This serves to enhance targeting of true ‘needs’, focused solutions, and the eventual uptake of resultant technologies. Both necessity and creativity incentives align around the concept of Value-Based Design. Even where challenges or technology foci are unique to either a high income or low income setting, these processes of innovation can be enhanced by participants from the entire range of settings by virtue of their unique preferences, skills or incentives. According to Donald Berwick, to optimise diffusion of innovation, an infrastructure must be present that allows ‘slack for change’, or an investment of time, space and energy to generate ideas and connect key players in the innovation process.17
Developing innovation infrastructure for Co-Creation
The Consortium for Affordable Medical Technologies (CAMTech) supports development of technologies that are clinically impactful, technologically disruptive and commercially viable using the principles of Co-Creation. CAMTech is administratively based at the Massachusetts General Hospital (MGH) Center for Global Health (CGH) and is a consortium of institutions across India, Uganda and Boston. The initiative has undertaken a multipronged effort to create innovation capacity and entrepreneurial activity in and targeting LMICs. Given the increasing need for Value-Based Design for medical technology in HICs, this strategy is designed simultaneously to serve individual patients and the healthcare system through technologies with enhanced performance and populations through enhancing value, regardless of their national income settings.
The components of this approach include medical technology ‘Hack-a-Thons;’ critical juncture funding mechanisms or ‘Innovation Awards;’ intersectorial innovation hubs called Co-creation Laboratories; and business-accelerator and ongoing mentorship for promising projects through the CAMTech Online Innovation Platform.
Medical technology Hack-a-Thons are 2–3-day events that bring together engineers, clinicians, entrepreneurs and patients to initiate medical technology solutions contributing to improved health in LMICs. By maximising ‘unlikely pairings’, Hack-a-thons use the theory of crowd sourcing18 to develop solutions for critical clinical challenges. The Hack-a-thons have attracted over 1600 participants from academia, industry and the clinical sector. Since 2012, the hack-a-thons have generated 210 innovations, ranging from diagnostic tests (23%) to medical devices (33%) and mHealth (15%). Technologies have been created in the areas of infectious disease, non-communicable diseases, maternal and child health, road safety and others.
Further development of an idea is then facilitated through an Innovation Awards programme that supports the development of technologies through critical stages of the product development process. An expert Technology Review Committee (TRC) evaluates the proposals across the domains of potential health impact, technology feasibility and commercial viability. The TRC comprises clinicians, engineers, designer, and entrepreneurs who have extensive experience in medical technologies in LMICs.
Many new medical technologies have underdeveloped business strategies to permit the scaling that is required for ultimate health impact. Team participation in business accelerator programmes is henceforth facilitated very early in the technology development pathway. Partnering with accelerators in the USA and internationally helps to ensure that entrepreneurs are considering the sustainability of each technology from the onset.
Co-Creation Laboratories are innovation ‘hubs’ that are designed to develop critical innovation infrastructure. They permit the intersection of these various entities on an ongoing basis, creating physical infrastructures as both focal points for intense, short-term collaborations through hack-a-thons or educational programmes as well as longer term project meetings, prototyping and development activities. The Co-Creation Lab at Mbarara University of Science and Technology (MUST) is currently fully operational and hosts a multitude of technologies and entrepreneurs.
Co-Creation Laboratories also house CAMTech's Innovator-in-Residence (IIR) programme. The IIR programme invites mentors to spend an extended period of time within the healthcare settings and communities surrounding the labs. IIRs bring a variety of technical and commercial expertise to students, faculty and entrepreneurs who are working on products to address local needs as well as commercialisation of resultant medical technologies. IIRs play an important mentoring role of advising on management for early-stage technology development projects, participating in local ‘hack-a-thons’, holding seminars, lectures and engaging with the local ecosystem of entrepreneurs working on scalable and sustainable business models. CAMTech's first IIR, a mechanical engineer and entrepreneur, spent 3 months in residence in 2013 to help identify the components necessary to enable medical technology innovation for the Co-Creation Laboratory in Uganda.
Although administratively housed in academic institutions, this approach takes an agnostic view towards sourcing of promising solutions. The accelerator works with private for-profit companies, academic faculty and students, non-profit sector employees and delivery organisations, and individuals provide feedback and facilitation throughout the process. Unique collaborations are encouraged, and the development of novel, value-based solutions will be poised to address health challenges throughout the world.
In June 2015, CAMTech launched the CAMTech Online Innovation Platform at http://www.camtechmgh.org. The CAMTech Online Innovation Platform connects global health innovators with an extensive network of experts, entrepreneurs, investors, policymakers and end-users to accelerate the development and commercialisation of impactful innovations. The CAMTech Online Innovation Platform is addressing a critical gap in the medtech ecosystem by providing expertise, resources and targeted support to global health innovators.
Summary
Creating platforms that permit necessary capacity for innovation can accelerate medical technology innovation in HICs and LMICs. Investing in entrepreneurship and focusing on Value-Based Design from the perspectives of effectiveness, scalability, sustainability and, ultimately, health impact will be increasingly important as our world globalises. Partnerships between innovators in LMICs and HICs will benefit those in all settings through the process of Co-Creation. CAMTech provides an example model for a multipronged approach using linked concepts such as Hack-a-thons, Innovation Awards, Co-Creation Laboratories and Innovators-in-Residence to promote a new model for global technology development.
Footnotes
Contributors JWD and KRO drafted the initial manuscript. All authors conceived the paper and contributed intellectually to the work herein. All authors read and approved the final manuscript.
Competing interests None declared.
Funding All of the authors are affiliated with the Consortium for Affordable Medical Technology. This article was funded by the Bacca Foundation and the Omidyar Network. David Bangsberg also received support from MH K024 87224.
Provenance and peer review Commissioned; externally peer reviewed.