Article Text

Abstract
Much has been written about the symbolic function of the white coat: its implications of purity, its representation of authority and professionalism, and its role in consolidating a medical hierarchy. By contrast, the medical literature has paid almost no attention to the patient gown. In this article, we argue that in order to understand the full implications of the white coat in the doctor–patient relationship, we must also take into account patients’ dress, and even undress. We explore contemporary artistic images of white coat and patient gown in order to reveal the power differential in the doctor–patient relationship. Artistic representations capture some of the cultural ambivalence surrounding the use of the white coat, which confers professional status on its wearer, while undermining his or her personal identity. At the other end of the sartorial spectrum, hospital gowns also strip wearers of their identity, but add to this an experience of vulnerability. Although compelling reasons for continuing to wear the white coat in circumscribed settings persist, physicians should be mindful of its hierarchical implications. Ample room remains for improving patients’ privacy and dignity by updating the hospital gown.
- Doctor
Statistics from Altmetric.com
Much has been written about the symbolic function of the white coat: its implications of purity, its representation of authority and professionalism, and its role in consolidating a medical hierarchy.1–12 By contrast, the medical literature has paid almost no attention to the patient gown. Two studies on patient privacy and dignity mention in several short sentences that patients, but not nurses, include the gown as a factor contributing to indignity.13 ,14 Two qualitative Scandinavian studies based on interviews of a small number of patients conclude that patient clothing while convenient, also depersonalises and marginalises the wearer. Both studies acknowledge a striking paucity of research on the impact of patient clothing on patient and provider attitudes.15 ,16 This is somewhat puzzling, as the relative undress enforced by the patient gown exacerbates the status differential between doctor and patient, and may affect patients’ experience of the medical encounter more deeply than their response to what their doctors are wearing. Especially at their most vulnerable—during the physical exam and in the hospital—patients lose the right to any trappings of individuality when donning a hospital gown.
In this article, we argue that in order to understand the full implications of the white coat in the doctor–patient relationship, we must also take into account how patients dress.17 In particular, we use visual art as an interpretive source. In order to explore how certain artworks depicting medical clothing represent common attitudes and ambivalence towards medical status and hierarchy, we have identified a number of artistic representations of physicians’ and patients’ clothing. Some of these, such as ‘The Cloaking,’ or ‘Leapfrog,’ foreground the actual garments, while others use the clothing as one of several visual indices to make more general statements about physician and patient roles. Our selection process has involved finding appropriately representative images, particularly contemporary ones, through internet searches, inquiry among professional organisations and personal knowledge of artistic works. Additionally, we have selected images for which copyright permission could be readily obtained. The broader goal of this analysis is to show how the visual arts can contribute to our understanding of medical self-representation: the visual arts purposefully portray the medical hierarchy manifest in everyday practice and bring its hidden assumptions to conscious awareness. Paintings and photographs, thus, facilitate useful reflections and provocations, and serve as a potential teaching tool for new generations of medical trainees who will perhaps have increased freedom in choosing how to represent themselves.
The white coat: professionalism and the loss of identity
Although the jury is still out on a suitable dress code for physicians, fewer physicians today may be routinely wearing a white coat than in previous decades.18 ,19 Concern about contamination and changing norms are probable influences on a trend toward less formal wear.20–22 However, the symbolic and practical function of the white coat continues to hold sway for a number of reasons: physician attire imparts on the practitioner a professional identity; white coats reassure patients of their doctor's authority and help them identify doctors among a confusing array of medical personnel; white coats have convenient pockets and provide coverage of street clothes that make them practical for wear.23
We speculate that a degree of ambivalence has grown around the white coat ‘uniform’ because as a generic garment, the white coat confers professional identity at the expense of personhood, and this trade-off may no longer be acceptable to a newer generation of doctors.24 ,25
As an anchor for comparison, we begin with a historical representation of a physician portrait. In Winthrop Chandler's painting, his subject, Dr William Glysson does not wear a white coat. (For an internet-based image, see (http://www.ajronline.org/doi/pdf/10.2214/ajr.168.3.9057505).
Instead, he poses in elegant dress. He is wearing expensive cuffed leather riding boots that only the wealthy would wear. His red frockcoat, made with felted superfine russet wool and expensive silver-gilt buttons, was worn as formal day wear in Britain during this period.26 His legs are crossed, expressing aristocratic ease, and the perfectly vertical walking stick conveys authority and confidence of social station. The physician's self-displaying pose and clothing establish the physician's identity as a person of importance. The portrait emphasises his role as a ranking member of his social class, while his function as a physician is secondary.
Compare this now with a photograph by Andreas Schreiber (Untitled, figure 1).

Andreas Schreiber, Untitled, 2004 (photgraph provided by Andreas Schreiber).
In this pictorial, social identity is irrelevant. Schreiber's image does not profile any individuals. The physicians in Schreiber's photograph are literally the ‘white coats,’ as doctors are sometimes called. The wearers are interchangeable. We see little else of their physical attributes. Indeed, Schreiber's photograph shows the physicians’ loss of individuality as they participate in a professional hierarchy.
The uniforms’ glaring whiteness recalls other black-and-white photographs depicting medical environments, in particular a genre of historical black-and-white photographs peopled by doctors and nurses. (See eg, (http://www.history.navy.mil/photos/images/h52000/h52960.jpg) and (http://www.nlm.nih.gov/exhibition/aframsurgeons/pioneers.html#freedmen). But unlike formal or historical depictions of medical personnel, the personae in the modern photograph vanish and are replaced by generic occupants of professional roles. The physicians’ facelessness accentuates the impersonal nature of their presence as they crowd around and loom over the patient.
A number of other contemporary visual representations exploit the contrast between what might loosely be called professional importance and personal impotence. These images examine the white coat's symbolic function as a means of engaging with the question of role assumption, and of speculating deeply and thematically about the losses this step into professionalism might entail.27 ,28 Take, for example, the painting of a student receiving his white coat in a widely practiced inaugural ceremony. (‘The Cloaking’ figure 2)

Suliman El-Amin, The Cloaking, 2012, acrylic on canvas, 42×42 in. (1.07×1.07 m). Collection of the artist, Washington DC (photograph provided by Suliman El-Amin).
This painting depicts a student's ritual transition to professional status. He is assisted by two parental mentors, a man and a woman, whose supportive gestures encourage their offspring to take flight. Indeed, the student's arms are spread, the white jacket suggestive of wings or a sail. At the same time, there is perhaps some stiffness in the gesture, as if the fledging is not quite ready to soar. His gaze is slightly off-centre—not directed at the viewer, but into some hopeful future that the central figure nonetheless contemplates with an air of apprehension. The flanking adult figures may even convey a sense of crowding or coercion. To add to the scene's equivocal message, the white jacket is about to cover a bright blue shirt; only the knot of his imperfectly hanging pink tie will remain visible even after the cloaking. One speculates what the newly donned professional identity holds in store for this acolyte—is he giving up his identity as a person who wears bright shirts and pink ties? His facial expression is synchronised with those of both of his mentors, suggesting he has already assimilated the professional mask that conceals his true feelings.
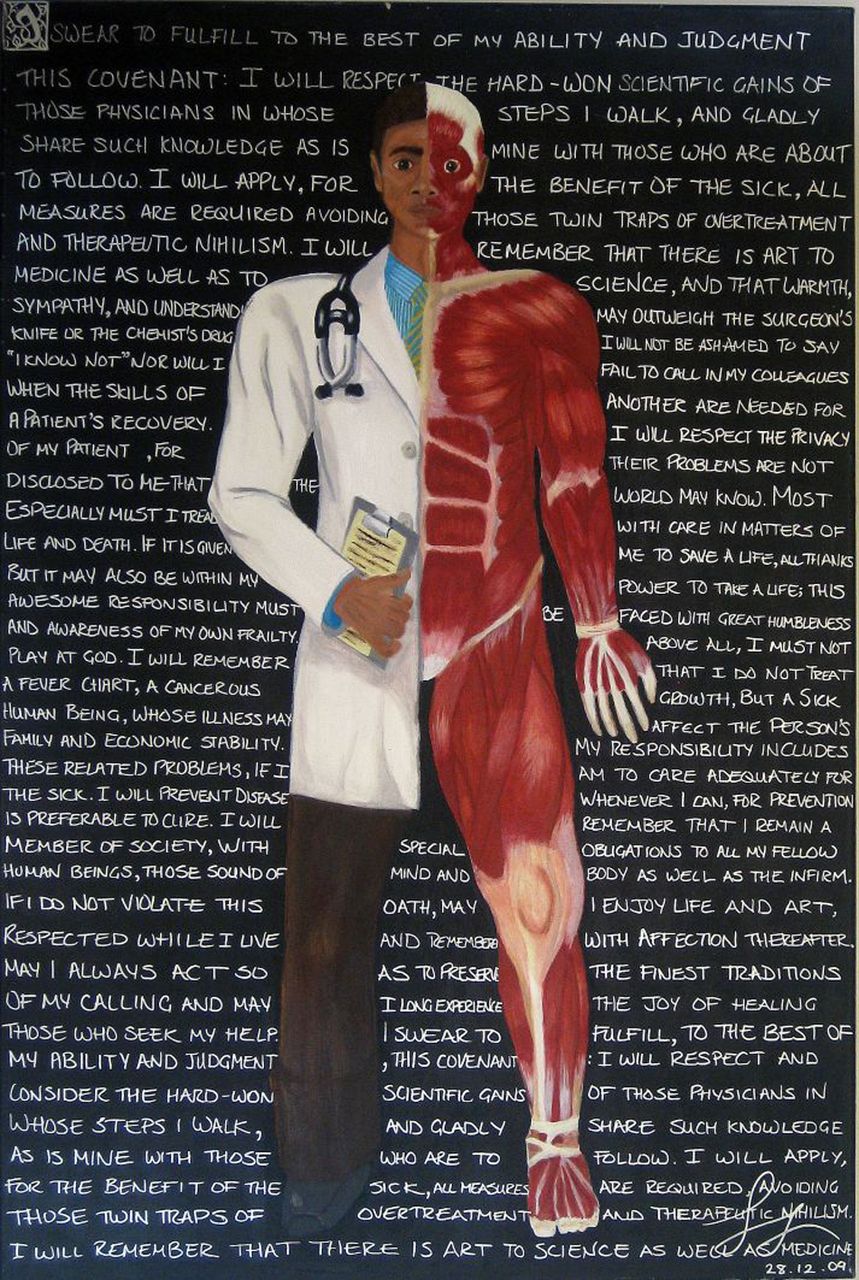
Another student painting also interprets the white coat's role in shaping professional identity. (‘All human,’ figure 3) The figure is divided vertically into two halves: one wearing the medical student's uniform—the white jacket—and the other exposing the anatomised body, which the subject has evidently studied to the point that he has physically assimilated it. What is glaringly absent here is the in-between self—the actual human being with any of the features through which the subject might construct a singular self. In this painting, too, the student's expression assumes a mask-like appearance. The only hint of emotion is that of wide-eyed surprise which, however, provides little reassurance regarding the professional enterprise, as one half of the effect is achieved through the hollowed-out eyes of a dissected body. As in ‘The Cloaking,’ the viewer catches a glimpse of a colourful shirt and tie. The viewer wonders if this is merely a part of the formal uniform or a small remnant of personal choice the artist wishes to represent on behalf of the student.

Sanjna John, All human, 2009, acrylic on canvas, 24×36 in. Collection of the artist, Ottawa, Canada (photograph provided by Sanjna John).
A written credo of sorts makes up the background. Presumably its well-intentioned sentiments reflect the medical student's hopes and wishes for himself. But there is also something in the words filling the background that provokes the viewer to suspect that they too are crowding out the student's personal self. There is no room for the student's own thoughts; instead, the professional mantra begins to repeat itself, its incantatory effect potentially representing the challenge of living up to the grand imperatives of medicine, but also invoking their rote nature.29
Physician attire in the medical hierarchy
Thus far, we have discussed the loss of personal identity that the physician assumes in donning the white coat. This phenomenon appears to be more pronounced in our contemporary understanding of medical practice than it might have been in the past when individual identifiers played a more prominent role in representations of physicians. This loss of personal identity, as we have seen, is especially noticeable in transitional moments, for example, when medical students officially assume their professional role. At the same time, all the images we have seen represent an ascension into or assertion of medical authority. Thus, loss of individual identity is the price to pay for professional gain and all the benefits—authority, status—it may entail.
We add to these observations a few words about the medical student's white jacket so prominent in ‘The Cloaking.’ The short white coat medical students wear has its own hierarchical connotations, to our knowledge rarely discussed in the literature.30 It is indeed part of the ‘hidden curriculum,’ in the sense that it connotes unspoken derogatory meanings. Historically, concomitant with the advent of the white coat, US medical students donned short white jackets, as seen in figure 2, and their coats become longer as they ascended the ranks of medicine.12 ,31 By examining the length of a person's coat, the patient or others can decipher the clinician's seniority and make assumptions about increased medical knowledge. The short white jacket may be seen as emasculating compared to the dignified full coverage of the long coat. Short coats were typically worn by women in the 18th century, compared with the long coats during this same period, as seen in Chandler's portrait of Glysson. In fact, these short jackets were called pet-en-l'air (‘fart-in-the air’) because they did not completely cover the buttocks. These factors contribute to a ‘long white coat envy’ further perpetuating a hierarchy.32
The patient gown: intimations of vulnerability
In several of the images discussed we see a depiction of a hierarchy, in which the patient is either absent or obscured. In the Glysson portrait and the Schreiber photograph, the patient is hardly visible. The Schreiber photograph, in particular, depicts a hierarchical superiority in relation to the patient. In the latter, the patient seems much diminished by the consulting doctors and the camera's downward angle. An arm reaching for the overhead handle obscures his features. The patient, like his doctors, experiences a negation of identity, but he lacks the compensations their role affords.
The patient gown, like the white coat, designates a transition covering or negating personal identity; in the case of the patient, donning the gown inaugurates the patient into his or her sick role. According to one study using patient interviews, hospital clothing is not only a metaphor for illness, but a way of designating the lowly status of patients because of emphasis on caregiver convenience over attention to fit, coverage and aesthetics.33 The portrayals of uniformed physicians contrast sharply with images of patients’ dress or, in fact, ‘undress’. While the white coat covers the wearer's personal clothing, the patient gown covers nakedness, and nakedness, interestingly, is a powerful expression of connection and raw identity.
The possibilities nakedness invites is conveyed in ‘Patients,’ one of Nicholas Nixon's photographic series, depicting subjects comforting sick loved ones, skin on skin. (See eg, ‘John Grady and Tessair Lauve’ Cambridge, 1997, ‘Susanne Richardson and her husband Barry Donner’ Dorchester, Mass, 2005; ‘John Royston and Jorge Armesto’ Easton, Mass 2006. In a similar vein, Melissa Chan's line drawing (figure 4) represents a young man carrying an ailing figure—the Chinese characters flanking the image depict the words ‘healer’ and ‘physician,’ their symmetrical placement conveying their parallel meanings. Nothing could contrast more sharply than these images with those we have just viewed: in Nixon and Chan's patient–caregiver dyads, the subjects are stripped of clothing. Their nakedness expresses the radical intimacy of their relationships. In fact, nothing comes between them. In the Chan image, one continuous line connects the figures, while the line's hiatus at the level of the heart signifies their intimate bond. The patient–caregiver's respective vulnerability and tenderness offer the viewer a glimpse of an authentically motivated model of care. Contrast this with the provider-focused lens of the photographs and paintings just discussed. Their subjects emanate—and in some instances also raise questions about—the pride, authority, and power their positions confer upon them. These physician-centred images say a great deal about medical identity, but reveal almost nothing about how this identity relates to care-giving.34

Melissa Chan, The doctor, pen and ink. Collection of the artist, Albany, California (photograph provided by Melissa Chan).
Images of patients’ dress or nakedness tell a story of exposure and vulnerability. The gown is a counterpart of sorts to the white coat—a deidentifying uniform which requires that patients wear identifying bracelets, just as physicians wear self-designating white coats and photo IDs. Unlike the white coat, however, which confers protection, status and authority, the patient gown signifies exposure, submission and humiliation. Recognising these potential effects, some researchers and hospitals have made efforts to improve gown design.35–37 These campaigns have responded to complaints about the poor bodily coverage and the unattractive design of gowns.
These elements of vulnerability are visible in several artworks we located that incorporate patient clothing into their theme. One medical student artwork, ‘Stormy Unveil,’ depicts a patient floating through an ethereal substance. (figure 5) According to the artist, this work interprets the patient's trust in the physician through such acts as disrobing.38 We cannot help but contrast the patient's fluidity with the medical student's awkwardness in ‘The Cloaking.’ The floating conveys a dream-like state that signifies the patient's unmooring, occasioned in illness by the loss of familiar coordinates and anchoring features in the surrounding environment. The subject's floating state in this painting conveys a sense of the patient's vulnerability, as does her fluid drape. The patient's ‘clothing’ is a scarf providing little coverage of her nakedness. All the patient can do to protect herself from this exposure is to close her eyes.

Ying Wei Liu, Stormy Unveil, 2010, acrylic on canvas, 12×20 in (photograph provided by Ying Wei Liu).
At the same time that it depicts vulnerability, the art of the patient gown also strives consistently to redeem the patient from the soullessness of his or her condition. The patient in ‘Stormy Unveil’ is shown as young and whole and lovely—an idealised image, no doubt, but striking in its physical and psychological elevation of the patient compared with the crushed, obscured patient in the Schreiber photograph.
Interestingly, another work, an installation, also draws on the concept of floating to convey the patient's experience. The installation shows disembodied gowns suspended from the ceiling, circling in the ambient air currents like so many ghosts. (‘Leapfrog,’ figure 6) Their wispy substance seems to suggest the patients’ fragility as well as their utter invisibility, as though the gown—or their ghost-like supports—were all that remains of them. Disembodied clothing has a particularly haunting effect, as we know from collections of shoes assembled in Holocaust museums, to draw on a particularly stark example, or of clothing that serves as a memorial to the departed as evidenced in the work of Christian Boltanski and Chawky Frenn.39–41 The artist adds dimension to this interpretation by highlighting the whimsical side of her installation, as expressed by its title, ‘Leapfrog.’ Like the physician images evoking potentially positive attributes of physicianship and its darker attributes, so too are these patient images multilayered, conveying personhood on the one hand through evocations of humour and beauty, while depicting patients’ exposure and vulnerabilities on the other. But the chasm between physician professionalism and patient personhood remains. The images of white coats provoke speculation about the individuality they conceal, whereas the images of gowns explore the patients’ intimacies they expose.

Sumita Kim, Leapfrog, 2007, mixed media (hospital gowns, wire, and acrylic medium). Installations of various sized hanging pieces, average size: 36×48×24 in (photograph provided by Sumita Kim).
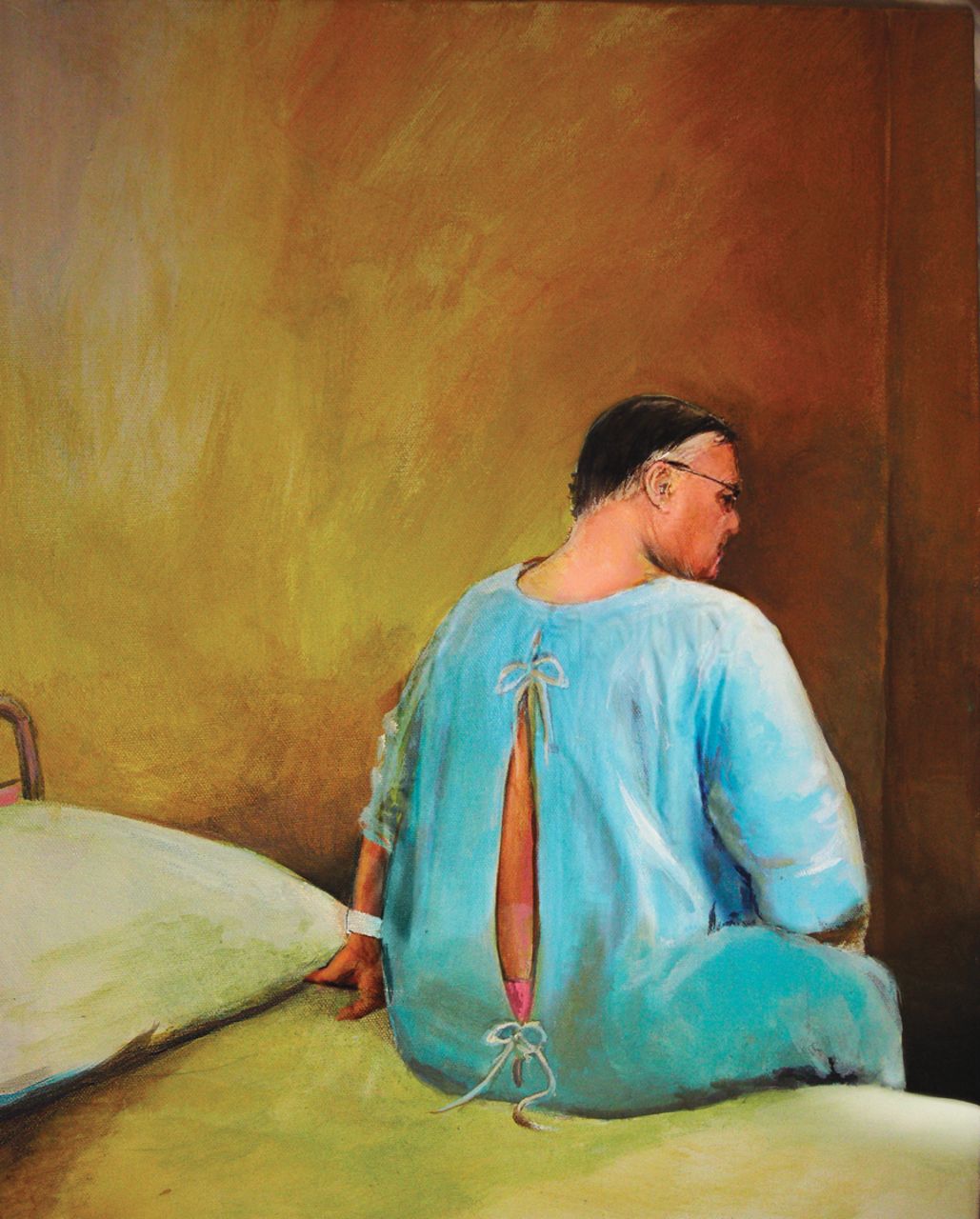
As a final example of patient dress as emblematic of patient vulnerability, we reproduce here Charles Sanderson's ‘Sick in the head.’ (figure 7) The painting depicts a seated middle-aged patient viewed from the back. He is wearing a hospital bracelet and the openings of his gown reveal a pink swatch of underwear. An initial interpretation links the viewer to ‘The Cloaking,’ in which the subject sports a pink tie. Is this underwear a hint of the wearer's identity—all that remains after he has been stripped of his clothes? Is this a wistful commentary on the patient's whimsical personality or sartorial fancy? The artist sheds further light on this work by commenting: ‘The painting is actually of Sheriff Joe Arpaio, a controversial sheriff in Phoenix who makes his prison inmates wear pink underwear.’42 Thus, we see that the patient is indeed even more disenfranchised than it initially appears—even the pink underwear is mandated by authority, a disenfranchisement that the artist turns on its head by representing the perpetrator as the victim of his own ordinance. This mischievous, and even acerbic inversion suggests that those in power may soon be stripped, literally and figuratively, of their authority, and holds out hope that those in vulnerable positions may in turn be given a voice. See (http://srxa.files.wordpress.com/2013/04/hospital-gown-empathy.jpg).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Charles Sanderson, Sick in the Head, acrylic on canvas, (photograph provided by Charles Sanderson).
The artist, by provoking the viewer, facilitates this reflection, and invites the viewer to consider translating his or her conclusions into mindful action.
Conclusions: reflection and practice
From these close analyses of artistic representations, which highlight the very different meanings adhering to the white coat and patient gown, can we draw any conclusions for education and practice?
From the perspective of reflective engagement, the visual arts have a particular capacity to promote mindfulness, and at least part of this effect relates to the open-ended nature of the image. It does not tell the viewer what to think.43 Because of this apparent absence of a moral anchor, John Carey devoted his diatribe What good are the arts? to a deconstruction of the visual arts as an educational and ethical force, favouring instead literature for its ability to articulate an instructive purpose.44 However, a recent movement in arts observation suggests that paying close attention to visual art can hone clinical skills, promote mindfulness and enhance empathy. Thus, even when there is tension in the interpretation of a given work, as is inevitable in the images just discussed, the process of visual information-gathering itself has powerful potential, in particular, by serving as a precursor to reflection. Specifically, by careful scrutiny of images of doctors and patients in traditional medical garb, the observer questions his or her own assumptions about a uniform that might have been invisible otherwise. The visual representation forces the viewer to look at what, unframed, goes unseen. As part of the reflective experience, literary works can enhance or clarify visual provocation. As John Carey suggests, poetic language may be held more readily accountable for how it is interpreted, but its more engaging role for adult learners in multidisciplinary reflective activities is to reinforce or serve as a counterpoint to other artistic and experiential ambiguities. Regarding the white coat, a poignant example supporting the interdisciplinary dialogue between visual and literary reflection is John Stone's well-known poem, ‘Talking to the family.’ In this poem, Stone uses the image of the coat to convey the tension between the personal and professional. The physician dons his white coat to deliver bad news to the family—the coat protects him against his own vulnerability, and gives authority to his devastating message. His return home to replace a light bulb, in contrast, implies his defenceless humanity. These tensions and ambiguities within and across the visual and literary arts, encourage the adult learner to reconsider everyday givens.45–54
On the practical front, questions and controversies about wearing the white coat are not new. Certainly some attitudes towards medical garb have seen dramatic reversals. Before Joseph Lister introduced asepsis, surgeons gloried in ‘their good old surgical stink,’ and refused to change their surgical aprons.55 ,56 Since then, the white coat has served as a symbolic buffer against contamination, whereas more recently, concerns about contamination have led wearers to shed these traditional uniforms. In our era of complexity, we must satisfy ourselves with nuances, which take into account a trend toward increasing informality and greater interest in reclaiming personal identity, as well as a greater demand for physician–patient partnership rather than the old paternalism. While there may be no single dress code to satisfy the particulars of every situation, physicians should be mindful of the hierarchical statements implied by their garments and individualise their sartorial decisions contextually.
It may not be feasible to retire the white coat in every setting, nor is it possible to work around street clothes on every occasion, but we have the opportunity to give patients better options of wear. Liver transplant patient Richard McCann has noted that he wears a silver medical alert bracelet, because he wants to be seen as the kind of person who values himself. As a patient with longstanding medical needs, he has struggled to dignify his standing relative to his medical peers as expressed in an interview segment on equalising the physician–patient relationship.57 Allowing patients greater choice in their medical encounters (eg, by wearing their own loose-fitting clothing during hospitalisation), and developing and disseminating a more aesthetically affirming, more dignified patient garment may be patient-centred options in our institutional quest to equilibrate the doctor–patient relationship.
References
Footnotes
-
Contributors CW and MC contributed substantially to the design of this paper and were involved in the drafting of text and acquisition and interpretation of appropriate images. Both authors approved the final version being submitted and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.