Article Text

Abstract
Patients and family caregivers tell different stories about their illness and care experiences than their physicians do. Better understanding of the relationships among these narratives could offer insight into intersections and disconnections in patient, caregiver and physician perceptions of illness and care. Such understanding could support enhanced patient-centred care in medical education and practice. Narrative writing is increasingly common among physicians, patients and caregivers and uniquely positioned to reveal matters of concern to these groups. We conducted a scoping review to identify literature in which first-person narratives from more than one group (physicians, patients and/or caregivers) were considered as ‘data’. A search strategy involving nine databases located 6337 citations. Two reviewers independently screened titles and abstracts. Full-text screening followed (n=82), along with handsearching of grey literature and bibliographies. Of these, 22 met inclusion criteria. Most pieces analysed narratives by patients and caregivers (n=13), followed by patients, caregivers and physicians (n=7) and patients and physicians (n=2). Only nine pieces compared perspectives among any of these groups. The rest combined narratives for analysis, largely patient and caregiver stories (n=12). Most of the 22 papers used descriptive content analysis to derive themes. Themes of humanity, identity, agency and communication intersect between groups but often manifest in unique ways. What is absent, however, is a more interpretive narrative analysis of structure, orientation and characterisation within these narratives, which may reveal even more than their content. This scoping review offers a cautionary tale of lost potential. Many narratives are gathered and analysed but usually only thematically and rarely comparatively. We call for researchers to explore the potential of comparative analysis and the power of narrative inquiry in the field. Comparative narrative analysis may enrich understanding of how differences between perspectives come to be and what they mean for the experience of illness and care.
- review
- narrative
- physician
- patient
- caregiver
- analysis
Statistics from Altmetric.com
Introduction
A worrisome gap exists between patient and family caregiver perspectives and the perspectives of physicians on their respective experiences of healthcare and illness.1–9 This gap has been attributed to many factors, including interpretation, vocabulary, communication and culture.5 6 10–13 This gap matters because compassionate, empathetic patient care relies on achieving a shared understanding of illness and its meaning. To help bridge physician, patient and caregiver experiences of illness and care, we must first understand what is currently known in the literature about the intersections and divergences between their respective perspectives. We thus chose a scoping review methodology to gain comparative insight into the meanings physicians, patients and caregivers make of illness and care experiences.
Narrative is one potential source of such insight. Narrative provides a distinct ‘mode of thinking’—‘of ordering experience, of constructing reality’ that is interpretive and rooted in ‘the particulars of experience located in time and place’ and in specific cultural contexts (Bruner, p. 13)14, (Martin, p. 49).15 Through narrative, physicians, patients and caregivers can reflect on and make meaning of their respective experiences. By engaging with these narratives, others can also come to know—and empathise with—the ‘particular meanings and interpretations’ that the writers ascribe to their experiences (Bruner, p. 13)14, (Martin, pp. 49–50).15–19 In this scoping review, we therefore drew on research that considered narrative as a source of data to understand multiple perspectives on illness and care experiences.
Specifically, we reviewed research that considered first-person written narrative as a source of data. A first-person written narrative is a written representation of an event or sequence of events told from the perspective of the writer.20 21 Charon and Hermann contend that writing ‘unlocks reservoirs of thought or knowledge otherwise inaccessible to the writer’ and that ‘[r]epresenting one’s experience in language is perhaps the most forceful means by which one can render it visible and, hence, comprehensible’ (p. 6).22 In this view, writing yields unique insights and enables a given experience to be ‘apprehended and then comprehended’ by both the self and others (Charon, p. 6).22 Written narratives may thus reveal something ‘more’—something essential—that may be difficult to express in spoken interview responses, for example.23 The use of first-person written narrative is increasingly common among physicians, patients and caregivers and uniquely positioned to reveal matters of concern to these groups. Reflective writing, in particular, is increasingly accepted and used in medical training and practice.22 24–31 Its prominence stems from literature suggesting that reflective writing is a tool to nurture reflective capacity—the ability to review, interpret and understand experiences in ways that achieve deeper meaning and guide future behaviour.25 32 33 Underlying its use is the conceptual assumption that writing, in and of itself, enables people to reach a ‘state of reflection’—that ‘writing is how one reflects on one’s experience’(Charon, p. 6).22 Developing reflective capacity in physicians may foster improvements in empathy, communication, collaboration and professionalism16 25 34–42—skills that are central to the patient experience, quality of care, cost of care and physician burnout.39 43–45 Studies have also considered the increasing use of first-person written narrative among patients33 46 47 and caregivers,33 46 suggesting that it has an overall positive impact on mental and physical health36 and quality of life.46
Through this scoping review, we aimed to understand how first-person narratives from more than one group (physician, patients and/or caregivers) have been brought together in research to explore intersections and disconnections among them. For instance, we sought to understand the extent to which comparisons were drawn between groups, the analytical approaches used and the nature of the similarities and differences analysed as a result. Through this scoping review, we also aimed to identify gaps, limitations and missed opportunities in the current literature, thus informing future research directions.
First-person written narratives provide readily available data for analysis around a question of interest, and these data can be analysed in terms of what both its content and its form may reveal about the experience of illness and care. Researchers can look to a variety of sources for these narratives, including both pre-existing narratives generated spontaneously (such as blog posts) and triggered narratives produced as part of a research design (where writers receive instructions and/or a writing prompt as participants in a study). We anticipated that including a range of types of narrative writing in our scoping review might reveal different aspects of the illness and care experience.
Because we were interested in literature that explored intersections and disconnections in the healthcare experience, we specifically sought work that considered at least two perspectives. The narratives of each group can offer a distinct perspective on a shared illness and care experience: ‘What is evident is that the events or symptoms do not carry the same meanings when they are framed differently or viewed from different perspectives’7–9 (Raoul, p. 6).48 ,49 Our inclination to bring these perspectives into conversation with one another reflects applied work in narrative medicine where ‘combinations of caregivers, patients, clinicians, and other staff’ write, tell and receive stories in common spaces and where ‘the process of listening to themselves and to each other reveals the humanness in common of patient, caregiver and professional’ (Stanley, p. 46).33 Moreover, narrative is increasingly taken up by interdisciplinary scholars as a way for healthcare professionals to gain a deeper understanding of patient and/or caregiver experiences8 (Charon, p. 308)19 49 (Schleifer, pp. 1–2).50 Our scoping review explores to what extent and in what ways this motivation for using narratives in medicine has manifested in research that brings these multiple perspectives together. Building from this, we posited that reviewing literature that attends to written narratives by different groups side by side would illuminate points of connection and shed light on how different perspectives can create challenges for achieving a shared understanding of illness, as well as offer insight into how researchers have exploited the potential of such data.
Method
We conducted a scoping review to address the following research question: how have first-person written narratives from various combinations of physician, patient and caregiver sources been used to understand areas of intersection and disconnection among their respective illness and care experiences? A scoping review is a process to summarise and synthesise knowledge on a topic—to examine the ‘extent, range and nature of research activity’ (Arksey, p. 21),51 to map the literature ‘with the aim of informing practice, programmes and policy and providing direction to future research priorities’51 52 (Colquhoun, p. 1291)53 A scoping review assesses the relevance of studies in relation to a broad research question, rather than assessing literature for inclusion based on quality, as in a systematic review.51 No such review has previously been undertaken on this subject.
Inclusion and exclusion criteria
We held an initial team meeting (TM, JC, CW, LL) to discuss inclusion and exclusion criteria. For this scoping review, we included English-only results, with no restrictions on the date of publication. We included studies whose data sample included first-person written narratives on an illness or care experience. More specifically, we included literature that sought to analyse these written reflections (as opposed to literature that, in and of itself, constituted a written narrative, for instance) by any combination of at least two of our interest groups: physician–patient, physician–caregiver, patient–caregiver and physician–patient–caregiver. We defined ‘physicians’ as practising medical professionals including medical residents and medical interns. We understood ‘patient’ to constitute an individual receiving or who had received medical care. For ‘family caregivers’, also referred to as ‘informal caregivers’,54 we included parents, spouses, other family members or friends who ‘provide care [e.g. instrumental or emotional assistance54] to those who need supervision or assistance in illness or disability’, whether ‘in the home, in a hospital, or in an institution’ (Van Durme, p. 493).55 We excluded results pertaining to professional and formal caregivers, such as nurses.
Data collection
With the assistance of an information specialist (JC), we developed search strategies to identify research that included in its data set written narratives by at least two of our interest groups. Our search strategies used database-specific headings and keywords for writing, storytelling, physicians, patients, caregivers, illness experience, care experience and analysis. Each strategy was modified to complement the specific database and platform. The full search strategies for MEDLINE and Embase are included in the online supplement (online appendix A). The process was iterative, with search terms and sources refined to ensure more sensitive yet comprehensive searches of the literature. One author (JC), a health sciences research librarian, implemented the database searches in November 2016 and updated the search in March 2017. This search involved ABI Inform/Global Research (ProQuest) (1971–March 2017), Canadian Electronic Library (Canadian Health Research Collection and Canadian Public Policy Collection), CINAHL (EBSCO) (1981–March 2017), Cochrane Library (Wiley), Embase Classic+Embase (Ovid) (1947–March 2017), MEDLINE In-Process & Other Non-Indexed Citations, MEDLINE Daily and MEDLINE (Ovid) (1946–March 2017), Published International Literature on Traumatic Stress (ProQuest) (1871–March 2017), PsycInfo (ProQuest) (1806–March 2017) and the Web of Science Core Collection (Clarivate Analytics) (1900–March 2017). The search strategy further included handsearching of abstracts in conference programmes that we identified as related to our topic: Creating Space Symposium (2011, 2013–2016), Calgary Humanities in Health Care Annual Symposium (2013–2016) and The Examined Life Conference: The Writing, Humanities, and Arts of Medicine (2007–2015) as well as bibliographies of final selected articles. To ensure comprehensive coverage of grey literature, we searched ProQuest Theses and Dissertations, Networked Digital Library of Theses and Dissertation and System for Information on Grey Literature in Europe as part of our electronic search.
Supplemental material
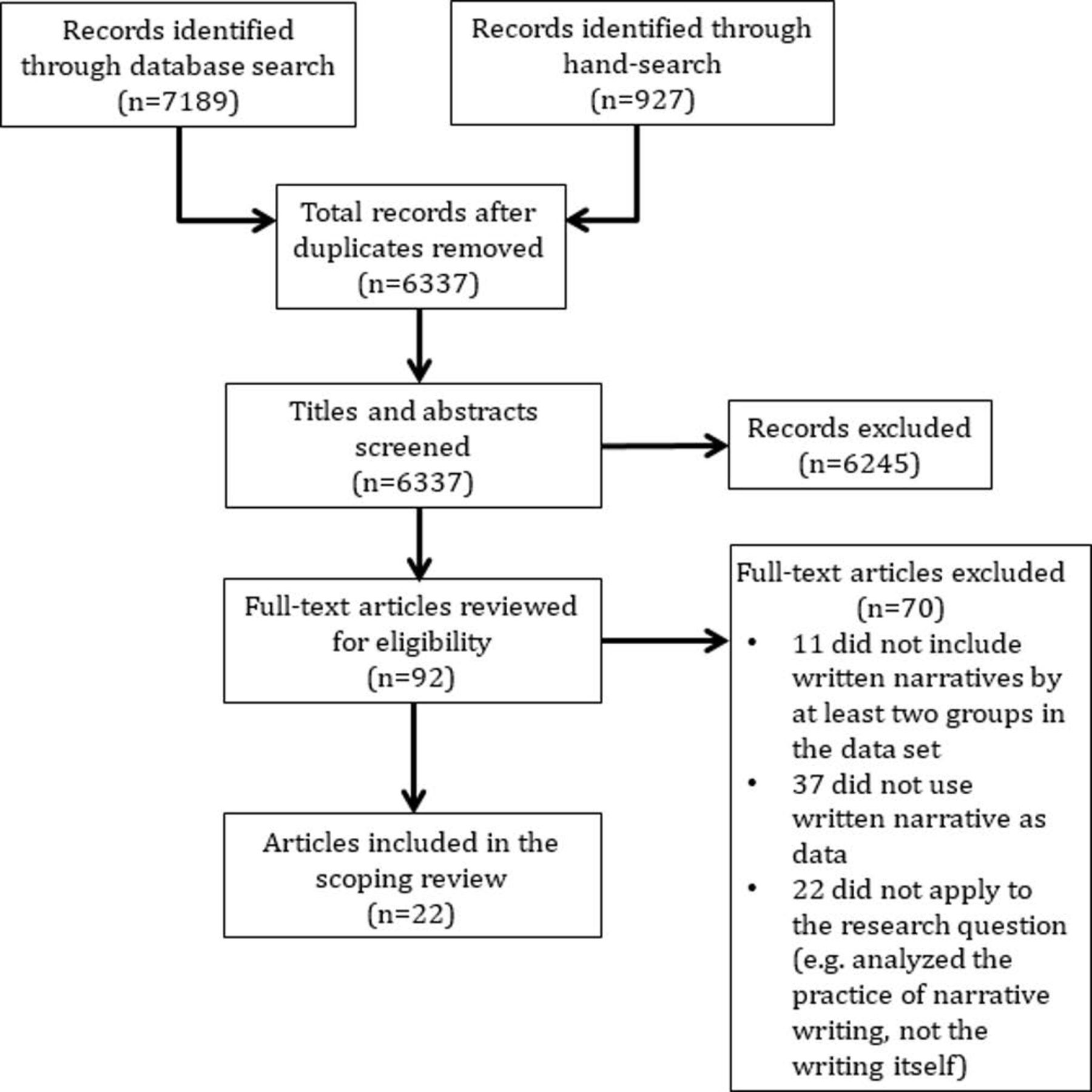
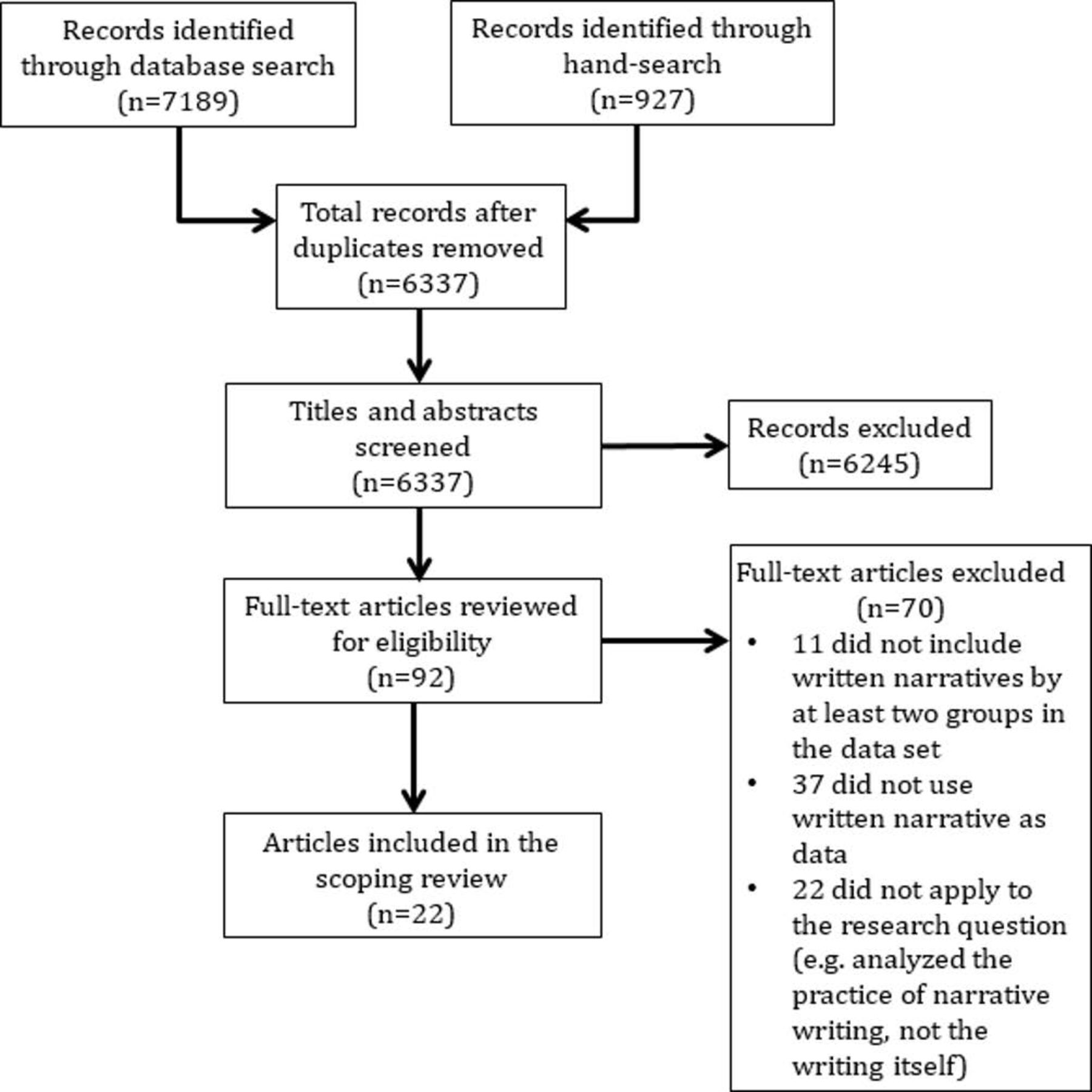
Figure 1 provides a flow chart of the article selection process. To organise the data, one author (JC) imported the records identified through the database search into Zotero and deduplicated the list. Two authors (TM, MG) independently screened each title and abstract of the records remaining after deduplication (n=6337), applying the inclusion and exclusion criteria. If it was unclear whether a study met the inclusion criteria, the citation was included for subsequent full-text review. The same two authors then reviewed the full text of the remaining records (n=92) to determine whether to include them in the final review. Any situations of disagreement on whether a citation should be included were resolved through discussion between the two reviewers to reach consensus. A third author was available to review if consensus could not be reached, but this step was not needed. In the end, 22 citations were identified for inclusion in the final dataset. A full listing of the literature included in this scoping review is available in the online supplement (online appendix B).
{kind=link}
Flow chart of the data collection and study selection process in a scoping review to identify literature in which first-person written narratives from more than one group (physicians, patients and/or caregivers) were considered as data.
Data charting and analysis
We (TM, CW, LL) collectively determined which variables to extract in the data charting and analyse to address the research question. Since data charting is an iterative process,51 53 we developed and piloted a data charting form on 5 of the 22 articles to determine whether the approach to data extraction fit with the research question and purpose. The same two authors who reviewed the citations to determine if they met the inclusion criteria (TM, MG) charted the data using the descriptive analytical method.51 We applied qualitative content analysis methods56 guided by questions such as: What was the purpose of the research? Whose perspectives were considered? Using what method(s)? Rationale and context for using written narrative? Type/form of written narrative? Similarities and/or differences in perspectives? Other results? We also tracked the disciplines and geographies of authors publishing in this area.
Our analytical framework further involved a thematic analysis of the statements of purpose and results reported for all pieces included in the scoping review. Because we were particularly interested in research that tried to exploit different perspectives to understand where they converged and diverged around healthcare experiences, we also conducted a thematic analysis of a subset of articles that explicitly compared perspectives across two or more groups.
Results
Descriptive findings
The earliest result was a journal article published in 1994, but the majority (68%) were published from 2010 onwards. Thirteen of the 22 pieces included in this scoping review were articles published in scholarly journals, and nine were abstracts in conference programmes (n=5) or in conference proceedings published through scholarly journals (n=4). Of the 22 pieces, 18 represented empirical work, one was a literature review and, of the remaining three pieces (all conference abstracts), two described panel discussions (not based on empirical studies) and one described a workshop.
None of the pieces explicitly defined narrative, but most authors cited a reason(s) for analysing narratives, often framing these narratives as representations of lived experience and a way to get a ‘look inside the mind’ of a population to enable an understanding of that population’s experiences and/or perspectives. For example, one study described the blog as ‘represent[ing] a unique, experiential account of the role of health in the lives of individuals’.57 The pieces did not offer an explicit rationale for analysing written narratives instead of other narrative forms. Some pieces grounded their methodological choice to use written narratives in the field of narrative medicine and its practice of reflective writing.58–62 The pieces included in this scoping review drew on different types of first person written narratives to apprehend physician, patient and/or caregiver perspectives, such as narrative anecdotes or essays (n=9), forum and/or blog posts (n=4), diary or journal entries (n=3), free-text responses (n=2) and letters (n=1). We included free-text responses because, in one case, the sample included longer form responses where participants were asked to ‘tell the story and describe the event in their own words’ (Jangland, p. 200)63 and, in the other article, the authors qualified participants’ responses to a prompt on a questionnaire—‘Please tell us about the main unanswered question or “uncertainty” you have about treatments for mental health problems. (If you wish, you may also provide a brief explanation.)’—as narratives in their stated objective to ‘understand the role of narratives in mental health research’ (Rapport, p. 373, 371).64 Some pieces (n=3) analysed more than one type of written narrative, such as one study that analysed blog entries, brief published narrative anecdotes and memoirs.58 The written narratives analysed in the journal articles and abstracts were equally divided between those that were naturally occurring (such as a forum post) and those that were produced as an artefact of research (such as a response to the writing prompt ‘Can you narrate about an encounter in health care that you found meaningful?’23).
Of the 22 scholarly articles and abstracts, the majority collected narratives by patients and caregivers (n=13), followed by those that collected narratives by all three groups (n=7), and then those that collected narratives by patients and physicians (n=2). None analysed narratives by physicians and caregivers only. In this scoping review, we set out to look at articles that collected narrative data from more than one group, but in terms of understanding the recurrent themes when comparisons were drawn between groups, only 9 (5 articles and 4 abstracts) of the 22 pieces included in this scoping review even attempted to make comparisons. The others amalgamated the narratives by two or more groups and treated them as one data set, even though there was distinct data from each group available. For instance, in the 13 articles that analysed patient and caregiver narratives, all but one amalgamated the perspectives. Overall, the journal articles and abstracts most often took a comparative analytical approach when physicians’ perspectives were involved, juxtaposing the analysis of physicians’ written narratives with those of patients’ and/or caregivers’. The two pieces that analysed physician and patient narratives compared their respective perspectives, as did most articles and abstracts that analysed all three groups. For this latter set (n=7), five pieces compared the groups independently (patient vs caregiver vs physician), one amalgamated patient and caregiver narratives and compared them with those of physicians and the remaining piece analysed patient, caregiver and physician perspectives together.
The scholarly pieces represented a range of geographic contexts, most notably the USA (n=10) and those international in scope (n=5) (eg, a sample of narratives drawn from an international journal or from a publicly available online forum), but also Sweden (n=2), the UK (n=1), Canada (n=1), Italy (n=1), New Zealand (n=1) and one based on narratives from sources in both the UK and Australia. We coded the disciplinary backgrounds of the authors based on their professional affiliations (eg, department) and credentials, as available. We observed that the body of scholarship under review reflected work by authors across disciplines and health professions and that many of the pieces reflected collaborative work by interdisciplinary and/or interprofessional teams. Broadly, the collection reflected a dominant medical/clinical viewpoint—authors with MD degrees or with ‘health science’ or ‘medical sciences’ affiliations as well as authors with other clinical expertise, predominantly nursing. Perspectives from the behavioural sciences, social sciences and humanities further contributed, with authors having backgrounds in psychology, sociology, social work, public health, law, business, hospitality management and fine art. The journals that published these works typically reflected a focus on clinical medicine, but we did not observe any repetition of journal titles publishing in this field, suggesting sporadic, disconnected publications rather than a robust conversation in a defined scholarly area.
All the journal articles based on empirical work reflected qualitative research (n=12). Of the empirical abstracts (n=6), one described a study with experimental design and the others used qualitative research methods. Overall, the most common methods used to analyse the written reflective narratives were content and/or thematic analysis (72%). Of the remaining five studies, one described its method as ‘consensual qualitative research, a methodology based on the principles of grounded theory’ (Kempainen, p. 207)65; another used a combination of content analysis and lexical analysis66; and three used narrative methods, specifically ‘modified narrative and visual rhetoric method’ (Grassau, p. 8),67 ‘hermeneutic narrative method’ (Gustafsson, p. 365)23 and ‘narrative content analysis’ (Rapport, p. 374).64 In addition to analysing written narrative, some studies (n=5) also employed other methods to address the research question such as survey research and analysis of audio recordings and arts-based images.
The qualitative content analyses focused on finding patterns or themes in the written narratives. For example, one article described a study that used content analysis to ‘better understand the needs and interests of [pulmonary fibrosis] patients and their loved ones … by systematically analyzing their engagement with the World Wide Web’ (Albright, p. 1).68 The researchers collected posts and responses to these posts from two blogs and one forum about pulmonary fibrosis developed independently by two physician-investigators with expertise in this disease, and they analysed the writing to determine why patients and family caregivers used the websites. The analysis revealed three patterns in why patients and caregivers use these interactive sites: (1) to share personal experiences (with the intent to offer psychosocial support or provide context to a question they sought to answer), (2) to seek information (about symptoms, diagnosis, prognosis, treatments, research, pathophysiology and disease origin) and (3) to offer a contribution to the pulmonary fibrosis community (about helpful resources, activities or behaviours). The researchers concluded by suggesting that clinicians should ‘encourage [pulmonary fibrosis] patients’ involvement in Internet forums that foster dynamic, bi-directional information sharing’ (Albright, p. 1).68 Similarly, a conference abstract described a content analysis of narratives about the burn experience written as part of a therapeutic writing workshop for survivors and their family members.69 The analysis derived 14 thematic categories, divided largely into negative and uplifting themes. Negative themes included negative mindset, negative emotions, pain, community disintegration, future fears and loss. Uplifting themes included positive mindset, cognitive search, identity recovery, positive emotions, community integration, journey and spirituality. From this, the researchers concluded that the thematic analysis ‘illuminated the depth of survivors’ experiences and their choice to express emotional memories of loss and recovery’, and it also gave ‘credence to the usefulness of group writing as a therapeutic outreach tool for aftercare of burn survivors and family members’ (Krueger, S250).69 Neither study attempted to compare patients’ stories with those of caregivers’ to explore differences in perspective. Furthermore, as these examples illustrate, the studies we reviewed that relied on content analysis considered only what was written—what the words themselves convey about the phenomenon under study. The content analyses operated at the surface of the text, taking the meaning of the words as self-evident and often rendering limited insights.
Narrative analysis, on the other hand, considers what was written and how it was written, including categories such as plot, characterisation, point of view and figurative language. Overall, the data set did not draw from the narrative tradition in the methodologies used. Of the three studies that did, one was an abstract that lacked detail about what the methodology entailed beyond stating that ‘[q]ualitative transcripts and arts-based images were imported into NVivo10 and were analyzed using a modified narrative and visual rhetoric methodology’ (Grassau, p. 8).67 The other two were papers that, respectively, described their use of narrative methods as narrative content analysis64 and qualitative explorative design with a hermeneutic narrative analysis.23
In the former, a 2010 study from the UK, researchers used narrative content analysis of open responses (to a questionnaire) by patients, caregivers and health providers (which included psychiatrists) to understand perceptions of uncertainty about the treatment of mental health.64 They ‘considered aspects of both manifest content and latent content through individual and group work over a 6 month period, honing data down to their major themes and categories’(Rapport, p. 374).64 The analysis revealed differences in writing style between patient and professional groups, identified perspectives unique to each group and highlighted three themes or areas of uncertainty shared by the groups: medication and treatment options, objectification and marginalisation of the patient and integrity of service delivery. While the study moved beyond analysing what was written to also analyse how the different groups told their stories, the contribution of the ‘how’ to the overall understanding of the data was limited. For instance, the study reported that patients often wrote in first person, told a story that integrated multiple questions and comments and used uppercase for emphasis, and that healthcare professionals often wrote from a third-person or ‘science-based’ perspective, posed specific questions and used little emphasis (Rapport, p. 375).64 However, the study did not delve into what these differences in writing style might mean in the context of the research question.
The second study that described its use of narrative methods was a 2013 Swedish study that analysed patient and next-of-kin stories about their experience of meaningful encounters in healthcare via a ‘qualitative explorative design with a hermeneutic narrative approach’ (Gustafsson, p. 363).23 The method included a structure analysis on two levels: (1) a broader analysis of narrative structure to interpret ‘how the patients and next of kin construct their narratives because this gives some indication of what is important and meaningful to them’ (Gustafsson, p. 366),23 and (2) a deeper analysis of the ‘plot within the plot’ focusing on ‘what the meaningful encounter expresses through metaphors found in the written narratives’ (Gustafsson, p. 367),23 given that metaphors may ‘reveal something essential in the narratives that may be hard to express in traditional interview answers’ (Gustafsson, p. 366).23 The analysis of narrative structure revealed four story forms for describing the meaningful encounter between a patient or next of kin and healthcare staff (which included physicians): (1) the gratification story (‘good examples of an excellent caregiver’), (2) the revelation story (‘a positive life-changing encounter’), (3) the documentary story (presents ‘a photograph of the current situation’ as if looking in on the encounter as a ‘witness’) and (4) the altruistic love story (idealised representation of healthcare staff ‘as a close altruistic important person to the family’) (Gustafsson, p. 367).23 The analysis of ‘deep structures’ revealed five metaphors to express the meaning derived from the encounter with healthcare staff: (1) steady rock in the stormy ocean, (2) it was like a warm wave, (3) we became as one, (4) as a fresh and healing hand and (5) she made me defrost. From this, the study concluded that ‘the meaningful encounter can be seen as a complex phenomenon with various attributes’ and that ‘[u]nderstanding the meaningful encounter will enable nurses to plan and provide professional care, based on caring science, focusing on patient and next-of-kin experiences’ (Gustafsson, p. 363).23 While the link between a more robust narrative analysis and a more meaningful result is not always clear, this study offers an example of how narrative inquiry methods can be used to take a deeper look at the process of storytelling and what this process can reveal about the relationships between physicians and patients or next of kin that can then increase our understanding of care and caring relationships. While this study did not attempt a comparison between patient and caregiver perspectives and, thus, did not explicitly explore differences in perspective, it did present an in-depth exploration of the patient and family perspective, with a message that understanding what constitutes a meaningful encounter for patients and families will enable healthcare professionals—nurses, specifically, were identified—‘to plan and provide professional care’ (Gustafsson, p. 363).23
Analytical findings
We analysed the statements of purpose across the 22 pieces for insights into how researchers have used first person written narratives to understand areas of intersection and disconnection among the illness and care experiences of physicians, patients and caregivers. What questions did they ask? Four inter-related themes emerged: needs assessments, best practices, vicarious knowledge and methodological or pedagogical utility. Studies tended to analyse written narratives to gain insight into the needs and interests of (predominantly) patients and caregivers during the illness and care experience. For instance, one study analysed open-ended responses on a questionnaire and prompted pieces of writing to ‘obtain information about which support resources were considered to be of greatest need by [Parkinson’s Disease] patients themselves and their caregivers’ (Gross, p. 36).66 Studies also analysed writing to determine best practices in patient-centred care by considering what worked and what did not work according to patients, caregivers and physicians. For example, one conference abstract described a study that, through thematic analysis, ‘explore[d] the meaning and value of the narrative of letters of gratitude (received from patients and families) and the association with an interdisciplinary team approach to cancer care’ (D’Angelo, p. 361).70 The theme of ‘vicarious knowledge’ embodied literature that used written narratives as a way to, as one study described it, ‘develop an explicit framework for understanding what it feels like to be a health care recipient’ (Kempainen, p. 207)65 or, as in other studies, a healthcare provider. The theme ‘pedagogical or methodological utility’ referred to research that set out to either ‘evaluate the pedagogical use of narrative for encouraging self-reflection and empathy in the hospital setting’ (Shafer, p. 125)59 or then ‘to explore the utility of qualitative research methods’ (Rapport, p. 371),64 for instance. Only one piece, a conference abstract describing an expressive writing intervention whose narratives were analysed through content analysis software, explicitly stated that its purpose was, in part, to ‘analyse differences and similarities in the constructions of cancer between patients and professionals’ (Cheli, p. 136).71 Overall, through the various purposes articulated, this body of literature reflects research that strived (whether implicitly or explicitly) to enrich patient-centred care through attention to quality of care and quality of life.
We also analysed the key results in the pieces that reported them (n=19) for patterns around similarities and differences between groups and recurring ideas among the content. We found that patients and caregivers often have different experiences, and caregivers tend to feel neglected in healthcare conversations—more like witnesses or outsiders to their loved ones’ illness experience or the ‘go-betweens’ for patients and healthcare professionals.63 64 Caregivers struggled to find their place. For example, with respect to integrity and service delivery, one study found that carers ‘felt frustrated and disempowered by the service in relation to medical supervision, advice and support…. Carers … considered that this forced them into a position of bystander or witness, whilst having to deal with some very negative side effects of prescription medication’ (Rapport, pp. 377–378).64 Across a number of papers, patients tended to feel objectified and marginalised within the healthcare system.57 59 Patients and caregivers alike expressed a need for greater psycho-social support, and they increasingly looked outside the ‘system’ at online communities to find this support.68 72 Physicians recognised the need to listen to and engage patients (eg, in treatment decisions) and understood that there is insight to be gained from patient perspectives.59 65 Broadly, patients, caregivers and physicians appeared to lack a sense of agency within the healthcare system, impacting their perceived ability to effect change in the direction of quality patient care.57 64 65 All three groups also grappled with issues of identity in their respective experience of illness and care. This included issues around a duality of selves, loss of self, recovery of self or transformation of self through the illness and care experience.58 65 73 Among the pieces, there was recognition of the centrality of professionalism, communication and advocacy to good healthcare delivery, as well as an emphasis on the importance of approaching care with compassion, empathy and hope.63 65 66 Finally, there was consensus that narrative writing offers a way for patients, caregivers and physicians to make meaning of their experiences and to understand the perspectives of others too.59 61 64 These themes, inferred from the key results reported, relate to the content of the narratives, not their structure. As noted, only three pieces—one conference abstract and two papers—explicitly used narrative methods. Thus, the absence of reported results relating to narrative structure reflects the paucity of narrative methods used to analyse narrative writing in these studies.
The use of comparison
We also looked at research that analysed written narratives between at least two groups to understand where they converge and diverge around healthcare experiences. Surprisingly, only five papers took advantage of the value of having data to potentially compare.58 59 64–66 Of these studies, two compared perspectives from all three groups,64 66 one compared patient and physician perspectives,59 one compared patient and caregiver perspectives (however, because most of these writers were also physicians, their narratives reflected this ‘dual role’ of physician-turned-patient or physician-turned-caregiver),65 and one amalgamated patient and caregiver perspectives and compared this set with the perspectives of physicians.58
We subsequently analysed this subset of five papers for a deeper understanding of their theoretical and methodological orientations and found that most papers did not give substantive treatment to either. Two papers grounded the studies, in full or in part, in the field of narrative medicine.59 66 Two papers anchored the methodological choices more generally in the suitability of qualitative analysis for research exploring people’s subjective experiences and their associated meanings.58 65 The final of the five papers also attended to the value of qualitative methods in health research, but it moved beyond this and drew on narrative theories—narrative as a way of knowing and telling—to justify its choice to study patient and provider narratives.64 Furthermore, most of the papers did not explicitly attend to the decision to comparatively analyse narratives by the respective groups.64–66 Rather, the comparative approach was inherent in the study objectives: ‘to identify aspects of uncertainty in mental health service users and providers’ (Rapport, p. 371).64; ‘to develop an explicit framework for understanding what it feels like to be a health care recipient and to explore how providers’ behaviors influence that experience’ (Kempainen, p. 207)65; and ‘to obtain information about which support resources were considered to be of greatest need by [Parkinson’s Disease] patients themselves and their caregivers’ (Gross, p. 36).66 The remaining two studies offered some insight into why comparative analysis was used. In one study, an explicit contrast to phenomenological approaches that ‘demarcate separate worlds of patient and physician’, authors sought to determine whether the use of writing could bring about some ‘overlap of these worlds’ (Shafer, p. 125).59 For the other study, taking a comparative analytical approach served as a check on reliability.58 The authors analysed caregiver and patient written narratives together in one data set to ‘create a truly dyadic representation of the experience of coupling post-[Traumatic Brain Injury]’ and then, as a method of data triangulation, they compared the emergent themes with those in physician-authored documents referencing the impact of TBI on coupled relationships (Godwin, p. 399).58
To understand the recurrent themes when comparisons were drawn between groups, we also analysed these five papers for more nuance of the similarities and differences in their results. Collectively, these five studies embodied the following dominant themes: humanity matters, identity struggles, lack of agency and communication challenges.
‘Humanity matters’ involved recognition of patient as person in the illness and care experience,74 and this theme manifested differently for each group. We identified three subthemes to qualify how each group related to the topic of humanity in healthcare: patient objectification, caregiver neglect and physician awareness. Patient narratives revealed feelings of anonymity, dehumanisation and marginalisation within healthcare systems.59 64 65 Caregiver narratives revealed feelings of neglect, both in terms of feeling excluded from discussions and decisions about care and feeling invisible with respect to receiving support in their new-found roles as caregivers.64 66 Patients, too, called for improved support programmes and services.64 66 Physician narratives suggested a recognition that the ‘science’ of medicine is overemphasised—at the expense of its ‘art’. At the same time, the literature also recognised that physicians empathise with patient fears and anxiety over illness and treatment and understand, to some extent, their own responsibility—and fallibility—in helping patients to feel seen and heard.58 59 All groups, but predominantly patients and caregivers, identified the importance of having a physician who acknowledges the patient’s humanity.64–66
‘Identity struggles’ were also part of each group’s narratives. Patients and caregivers wrote about a loss of individual and relational identities preillness—from healthy to ill, from wife to caregiver, from husband to dependent, for instance—as well as a need to develop new identities around their new roles.58 65 Physicians, when writing from the perspective of either a patient or caregiver, described this dual role as challenging and conflicting yet illuminating.65 Roles blurred and influenced each other, usually enhancing patient-centred care in their professional practice including ‘increased emphasis on communication…, newfound recognition of their ability to heal others, and/or greater empathy for patients and their families’ Kempainen, p. 210).65 When writing as physicians, they expressed insecurity and anxiety about competence in their practice, most notably about their ability to perform successful medical procedures that then help and heal patients.59
Patients and caregivers and, to a lesser extent, physicians expressed a lack of agency within the larger healthcare system—patients to advocate for themselves and to be supported through illness, and caregivers to support their loved ones and to be supported by the ‘system’ in the process.64–66 Patients and caregivers reported feelings of fear, anxiety and helplessness.58 59 64–66 Physicians, too, reported feelings of ‘helplessness’ (Kempainen, p. 208),65 along with ‘uncertainty’ (Kempainen, p. 208)65 and ‘loss of control’ (Kempainen, p. 211),65 which surfaced most prominently when physicians wrote from the dual role of either physician–patient or physician–caregiver. One physician-turned-patient wrote: ‘… I couldn’t believe that I was at the other end. I thought of the sick patients in the intensive care unit I had cared for so often with multiple lines going. Now I was on the receiving end of this life-sustaining device, and it was frightening’ (Kempainen, p. 210).65
All three groups noted issues with physicians’ communication skills. As one study found: ‘Essayists [patients and caregivers, many of whom were also physicians] noted deficits in both the quantity and quality of providers’ communication, including their ability to communicate coherently, humanely, and completely with patients, family members, and one another’ (Kempainen, p. 209).65 Patients and caregivers expressed the need for more communication and more comprehensive communication throughout the illness and care experience and identified the importance of having a physician(s) who advocates for the patient and family and who expresses compassion.58 59 64 65
Discussion
This scoping review set out to explore how first-person written narratives have been used to understand intersections and disconnections among the illness and care experiences of physicians, patients and caregivers. Our results tell a story about both the power and the lost potential of narrative. The universality of narrative gives it power. As Barthes wrote: ‘… there is not, there has never been anywhere, any people without narrative…. Like life itself, it is there, international, transhistorical, transcultural’ (p. 79).75 Through narrative, humans make meaning of their experiences, represent them through language—through ‘sequenced storylines, specific characters, and the particulars of a setting’—and often share them with others (Riessman, p. 5).21 Through narrative, we can understand the diverse and divergent experiences of others and the process of meaning-making behind the storytelling. The body of work we reviewed, however, does not meaningfully tap into the potential power of narrative, as it is limited both in the number of comparative studies and in the general depth of methodological approach to analysing these narratives, resulting in limited insights. In particular, our analysis yielded two novel findings: (1) although narratives from more than one group are often considered concurrently, comparative research is uncommon, and (2) analytic approaches focus on content, thus marginalising the very power of narrative as a data source. We elaborate on each of these key findings below.
The lack of comparative research
We looked for evidence of comparison across physician, patient and caregiver perspectives and found that most studies based on narratives from two or more of these groups did not take a comparative analytical approach. The health humanities as a field recognises the value of considering multiple perspectives—of bringing different perspectives side by side—and it recognises written narratives as a source of such insight.49 Yet, these studies did not leverage the value of having data to potentially compare. One explanation for this may be the dominant use of qualitative methodologies in the studies reviewed. Qualitative research emphasises context specificity, and key methodological texts in narrative research generally and narrative health research specifically either ignore comparative methods altogether21 76–79 or imply the importance of multiple perspectives without specifying procedures for exploring this multiplicity.80 Studies with experimental design are more often used to compare between groups, and the one study in our review with an explicit objective to compare perspectives between groups—‘to analyse differences and similarities in the constructions of cancer between patients and professionals’ (Cheli, p. 136)71—used a mixed methods approach, specifically experimental design via a psychometric questionnaire and content analysis.
This lack of comparative work represents a major gap in the literature. This gap matters because neither physicians, nor patients, nor caregivers are ‘individual actors in health care contexts’ (Clandinin, p. 94).81 To understand patients’ experiences, we need to understand the broader social and/or professional narratives that are unique to physicians and caregivers who are part of the patients’ healthcare teams and environments, and we need to understand how the narratives position these groups in relation to each other. The same is true of understanding the experiences of physicians and caregivers, respectively. This reinforces why it is problematic to blend patient and caregiver stories together for analysis, as did most of the studies we reviewed. As content analysis demonstrated, patient and caregiver experiences can differ.66 For instance, in a comparative study of patients with Parkinson’s disease and their caregivers, each group noted the need for different support resources.66 While patients emphasised their physical needs as most important, caregivers were foremost concerned with their own psychological needs. As in the case of this study, insight into differences between patient and caregiver experiences can inform the provision of tailored medical, psychological and social support resources and service to ‘lessen the burdens of illness’ (Gross, p. 36).66 There are also ethical issues with assuming a shared perspective among these two groups, especially in the context of a rich literature on the caregiver experience.82–85
The focus on content over narrative analysis
Most of the research identified by this scoping review is based on descriptive content analysis. Content analysis is a common approach to analysing qualitative data and, as our analysis of key results in this body of research demonstrated, this predominantly content analysis approach has proven helpful in yielding common threads of understanding where concerns and issues intersect and diverge between patients, caregivers and physicians. However, a more sophisticated narrative analysis might enrich understanding of how those differences come to be and what they mean for the experience of illness and care. Most of the published work acknowledged that we can learn from narrative but did not delve into questions that expose why we study narrative and what narrative can offer for analysis that is unique from other types of data collection. As noted, we found only two papers that attempted to tap into how the narratives were told and, to varying degrees, what this communicates about physicians’, patients’ and/or caregivers’ respective experiences of illness and care.23 64 However, even in these two studies, the contribution of the analyses to the overall understanding of the data and the conclusions derived from it was limited and lacked depth. Most of the published work did not exploit the fact that the objects of analysis are narratives—stories with plots, characters and points of view—that readily lend themselves to a more interpretive analysis that considers what these categories of storytelling can teach us about the illness and care experience.
We contend that there is a potential loss by focusing on thematic content to the exclusion of narrative structure and voice. Analysis of narrative structure ‘shifts the focus from the “told” to the “telling” and from exclusive focus on a narrator’s experience to the narrative itself’ (Riessman, p. 77),21 and while an analysis of narrative structure is also concerned with content, ‘attention to narrative form adds insights beyond what can be learned from referential meanings alone’ (Riessman, p. 77).21 For instance, in writing a story about a patient encounter, a physician can represent what happened in many ways. The physician’s specific choices in structure (ie, storyline) or voice (ie, point of view) offer insight into how the physician absorbed and made sense of a given patient care experience in context. As Nussbaum wrote: ‘The telling [of a story] … is not accidentally connected with the content of the told… No stylistic choice can be presumed to be neutral—not even the choice to write in a flat or neutral style’ (p. 245).86
Narrative inquiry also addresses some limitations of thematic content analysis—the assumption that ‘everyone in a thematic cluster means the same thing by what they say (or write), obscuring particularities of meaning-in-context,’ or the tendency to obscure ‘the investigators’ role in constructing the narratives [e.g., through writing prompts] they then analyse’ (Riessman, p. 76).21 Narrative inquiry offers researchers a way of interpreting human experience. As a methodology, narrative inquiry ‘deal[s] in human … intention and action’ (Clandinin, p. 90)87 and ‘attends to the relational aspects of living and telling stories, of context and person, of researcher and research participant’ (Clandinin, p. 91).87 Josselson and Lieblich wrote:
Through narratives we come in contact with our participants as people engaged in a process of interpreting themselves. We work with what is said and what is not said, within the context in which life is lived and the context of the interview [or written narrative] in which words are spoken [or written] to represent that life. We must then decode, recognize, recontextualize, or abstract that life in the interest of reading a new interpretation of the raw data of experience before us.88 (p. ix)
Narrative inquiry, thus, strives for a more in-depth understanding of human experiences and events through a process of analytical reflexive thinking. Most of the papers we reviewed did not look beyond ‘what is said’—beyond the literal meaning of the words—to consider ‘what is not said’. For example, one study analysed identity-related themes in published narratives by individuals with mental illness and their family members, with a goal ‘to understand and promote recovery from serious mental illnesses’ (Wisdom, p. 489).73 Narratives from both groups were analysed together, and five themes emerged: a loss of self, the duality of (ill/well) selves, perceptions of normality, concerns about parenting and identity, and hope and reconciliation. Overall, the analysis revealed a ‘loss of self and identity that had to be overcome, or at least managed, for recovery to become possible’(Wisdom, p. 489).73 To do so, the authors called for more ‘strengths-based patient-centred stories’ and concluded with the importance of foregrounding hope and recovery among patients, family members and clinicians (Wisdom, p. 489).73 While the themes usefully identified challenges around identity that may impact the recovery process, a narrative analysis could dig deeper into the different layers of meaning-making within a story—into the unspoken—that offer insights into how individuals ‘interpret themselves’ and their experiences. We could, for instance, analyse (separately, this time) the narratives of individuals with mental illness and their family caregivers for metaphors to understand and compare how these groups conceive of and symbolically represent their respective illness and care experiences. Or, what might an analysis of characterisation reveal about how individuals with mental illness construct the other ‘actors’ in their stories? These ‘actors’ may include family caregivers, members of healthcare teams and the illness itself (as personified by the patient). The same applies to the analysis of characterisation in family members’ narratives. Analysing point of view could further reveal how individuals with mental illness and family caregivers position themselves in the narrative and how they position themselves in relation to the other actors in their stories. Who is perceived to have—and to lack—agency? How is power enacted? To what end(s)? Such narrative approaches could offer a deeper level of insight into how identity is constructed, how relationships impact identity construction and how identity affects the recovery process.
Narrative inquiry has been underused in the health sciences, especially relative to thematic content analysis, and this paucity of research has implications for future work. There may be a lack of clarity about what narrative inquiry can offer to the health professions and to the sciences generally where ways of knowing rely on ‘paradigmatic knowledge’ and where methods tend to be quantitative and statistical and, as such, rooted in control, replicability, detachment and generalisation (Clandinin, p. 90).87 In contrast, ‘narrative approaches to understanding bring the researcher more closely into the investigative process’ (Josselson, p. ix).88 Historically, ways of knowing in medicine have strict boundaries, as Derkatch discussed in her exploration of the tensions between biomedical and alternative approaches to patient care and research.89 Where medicine is rooted in ‘basic sciences’, ‘evidence of safety and efficacy’ and ‘uniform standards of practice and care based on scientific research’, alternative ways of knowing attend to individual patient needs and contexts (Tucker, p. 139).90 Bruner argued that we need both paradigmatic and narrative ways of knowing to make meaning of the world and our place in it.14 15 Clandinin et al 81 highlighted some of the challenges in engaging in narrative inquiry within medical education research specifically, all of which have roots in the distinction between narrative and paradigmatic knowledge. One challenge is the contrast between methodological starting points—individual experience versus theory, respectively. Studies in medical education do not typically ‘follow from narrative inquirers’ ontological and epistemological assumptions’ (Clandinin, p. 93).81 Another challenge is to get physicians and medical learners ‘thinking with stories’, which necessarily involves ‘shifting attention from the more common practice in medical education of asking physicians and those learning to be physicians to write and think using clinical cases’, which rely on ‘objective biomedical data’ and exclude the physicians’ experiences (Clandinin, p. 94).81 The authors further cited ‘multi-perspectival narrative inquiry that attends to the experiences of multiple participants’ among the challenges in using narrative inquiry as a methodology in medical education (Clandinin, p. 94).81 One possible reason for this may be that narrative inquiry emphasises interpretation of others’ narratives, which are often context specific. What we learn from narratives in the context of one illness (such as Parkinson’s disease) is different from what we learn from narratives in the context of another illness (such as mental health). Similarly, what we learn from narratives told from the context of a patient’s life is different from what we learn from narratives told from the context of a physician’s life. How does the researcher apply a common narrative inquiry approach to analyse across perspectives that can be so different?
The potential of comparative narrative analysis
We contend that researchers can—and should—take advantage of the affordances of narrative and narrative inquiry, even in a comparative structure. In their discussion about multiperspectival narrative inquiry, Clandinin et al 81 focused on physicians and the importance of also considering the stories of other professionals that comprise the healthcare teams and work environments that physicians are a part of, as well as considering the larger social, institutional and professional narratives in which these individuals are embedded. Just as the authors argued that ‘physicians’ identities are shaped through stories they live and tell in relation to other allied healthcare providers’ (Clandinin, p. 94)81 so, too, have we argued in this paper that physicians’ stories are shaped in relation to patients and caregivers who also form part of the work environment, and vice versa with patients and caregivers. Literature in the health humanities further recognises the importance of attending to the perspectives of different groups on common experiences,7–9 49 91 and the need to bridge the gaps between these perspectives.9 49 Written narratives offer a window onto the illness and care experiences of patients, caregivers and physicians, and literature in the field of narrative medicine offers narrative itself—writing, telling and receiving stories—as a way to bridge these divides in medicine.17 18 33 49 91 Yet, there is a paucity of research that attends to these perspectives and identifies their commonalities and divides by analysing the narratives written by these groups side by side. While the literature suggests the value of a comparative approach, narrative-based health research does not readily apply this approach methodologically. Such an approach is, however, feasible. The 2013 Swedish study23 that used narrative inquiry offers an example of how researchers can analyse narratives with more attention to the form itself and in a way that relates to the process of storytelling that might offer useful comparisons. The researchers identified four key story arcs that respectively communicate something distinct about what constitutes a ‘meaningful encounter’ for patients and next of kin and five key metaphors that describe the ‘feeling’ attached to their meaningful healthcare encounter. Insight into the attributes that comprise a ‘meaningful encounter’ may enable healthcare professionals—in this case, nurses—to ‘plan and provide professional care, … focusing on patient and next-of-kin experiences’ (Gustafsson, p. 363).23 While the researchers chose to amalgamate the narratives of patients and their caregivers, they could have easily and readily extended this approach to compare how story arcs differ between both groups and what these differences might communicate about how these groups experienced an event. We maintain that there is promise in a comparative approach to analysing narratives by different groups, but the scholarship reviewed has not realised the full potential of this approach because of the tendency towards analytical simplification. While this may be attributed in part to perceived challenges with a comparative methodology, we see potential for more analytical sophistication even in a comparative structure.
Research from other domains can offer examples. A 2011 study in international business by Gertsen and Søderberg used methods and analytical techniques of narrative inquiry, specifically narrative interviewing and narrative analysis of plot structure, respectively, to study intercultural business collaboration.92 Researchers collected and comparatively analysed two accounts of the same series of events—one by a Danish expatriate manager and the other by his superior, a Chinese CEO, both working in a Shanghai subsidiary of a multinational enterprise. The narrative interviews probed at personal experiences of successes and challenges in intercultural collaboration, and the narrative analysis sought to ‘elucidate how [expatriate and local] managers make sense of and learn from critical events in their intercultural collaborations’ (Gertsen, p. 790).92 In their analysis, the researchers applied the narrative concepts of peripeteia (‘turning point’) and anagnorisis (‘recognition of hidden aspects of a situation that marks a change from ignorance to knowledge’) to identify focal points in the two stories—‘situations where change follows their recognizing new dimensions of their conflicts, eventually furthering their collaboration’ (Gertsen, p. 787).92 To analyse the plot, researchers then applied a narrative model, which breaks down the action that takes place in a story. Using this approach, the researchers ‘mapp[ed] differences between and changes in the narrators’ projects, alliances and oppositions in the course of their interaction’ to then demonstrate ‘how they overcome most of their differences and establish common ground through mutual learning’ (Gertsen, p. 787).92 Through attention to how an expatriate and a local manager constructed and developed their plots, with focus on situations where change, learning and progress occurred, this study demonstrates how a narrative approach can be applied systematically to data collection and analysis across two perspectives, capturing ‘insights not easily captured by other approaches’ (Gertsen, p. 802).92 While this study relied on narrative interviewing, the same narrative analytical approach could apply to stories collected in written form, and researchers could also consider a range of other narrative concepts (such as metaphor or point of view) to explore and compare the process of storytelling among different groups. This study offers an example to the health professions of how using narrative inquiry to analyse two different— even conflicting—perspectives can lead to unique insights and understandings.
Directions for future research
Future studies may consider whether the limited and often superficial use of narrative inquiry is related to the how the analysis itself is conducted, or to how the data are collected, or to the types of writing included as narrative data. While there is ‘no one common definition of narrative and agreed approach to its investigation’,93 one of the challenges to exploiting its potential may be the quality of the data categorised as ‘narrative’ in some of the studies. Some types of narrative data may be more nuanced and complex (eg, diaries) and, therefore, more suited to analysis of their storytelling approaches than others (eg, free-text responses in questionnaires). At times, the methodological choice to analyse written narratives in the literature reviewed did not seem well suited to the aims of the study. For example, with studies whose purpose was to conduct a needs analysis, survey research may have presented a more efficient approach to data collection. Narrative writing may also not be practical for patients and their caregivers who may lack the time, interest or ability to write about their experiences, and written narrative may be inaccessible to those who are already vulnerable to having their perspectives excluded, such as those with cognitive challenges or those whose first language is not English. Future research could explore what other non-written forms of narrative, such as conversations or photos, contribute to our understanding of multiple perspectives on illness and care experiences. More broadly, future studies could further explore methodological approaches to narrative inquiry and its concomitant utility to understanding the lived experiences of patients, physicians and/or caregivers. This would offer insight into the what and the how of narrative in a healthcare context and work towards filling a gap in knowledge within medical education research.
Overall, the limited comparative data suggest more commonality than divergence across patient, caregiver and physician perspectives, presenting an interesting point of departure for further work. Physicians, patients and caregivers identified a shared sense of the importance of humanity in medical care, offering a starting point for exploration of how humanity in healthcare is defined, enacted and experienced. Studies also revealed a shared sense that agency is elusive within the healthcare system, presenting an opportunity for exploration and conversation around how to effect change in what is often a frustrating and flawed healthcare system, even for physicians.74 Furthermore, while this scoping review focused on studies of physicians’ perspectives alongside those of patients’ and/or caregivers’, future research may wish to consider patient and caregiver perspectives alongside those of health professionals broadly defined or of a different group of health professionals, such as nurses. In all cases, attending to the narratives by different groups comparatively—using rigorous narrative analysis—will enable future work to tease out more nuanced insights into precisely where and how physician and/or patient and/or caregiver perspectives converge and diverge. Such insight will better equip medical educators, researchers and clinicians to leverage the similarities and address the differences in support of enhanced patient-centred care.
Conclusion
Our scoping review has demonstrated two fundamental shortcomings in how narrative data are treated in research related to patient, physician and caregiver perspectives on healthcare experiences: (1) the comparative potential inherent when narratives are collected from more than one group is often not exploited and (2) the distinct affordances of narratives in analysis are generally ignored.
Narrative is a powerful tool that offers something distinct, and we call for those looking to conduct research in the field to explore and exploit that distinctiveness through a more robust use of narrative data. We maintain that there is potential in a comparative analytical approach when using first-person narratives to explore the perspectives of more than one group on a healthcare experience. The narratives of patients, caregivers and physicians embody distinct perspectives and, analysed side by side, they enable insight into the points of intersection and disconnection in their perceptions of illness and care. We also offer a cautionary note about oversimplifying analyses of narrative data by considering the content only. Using content analysis with narratives misses the point of choosing narratives to study. In bringing these two insights together, then, future research that aims to compare written narratives across groups should draw on analytical techniques of narrative inquiry, which enable researchers to understand experiences of illness and care by looking at how people tell stories, how people position themselves within a narrative and what the key aspects of the story are. Comparative narrative analysis may enrich understanding of how differences between perspectives come to be and what they mean for the experience of illness and care.
References
Footnotes
Contributors All listed authors have met the ICMJE criteria for authorship. TM, JC, CW and LL were involved in the conception and design of the research. TM, JC and MG contributed to the acquisition of data. TM, MG, CW and LL contributed to the analysis and interpretation of data for the work. TM reported the research, and all authors were involved in revising the work. TM is responsible for the overall content as guarantor.
Funding This study was funded by a Mapping the Landscape, Journeying Together grant from the Arnold P. Gold Foundation.
Competing interests This project was made possible with a Mapping the Landscape, Journeying Together grant from the Arnold P. Gold Foundation.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.