Article Text

Abstract
There is now a context for teaching humanities in undergraduate medical education via special study modules (SSMs). This paper discusses the instrumental and non-instrumental role of the humanities in the education of doctors. Three courses are then described and compared. The most successful of the three is a SSM which had the following characteristics: it was voluntary, it was an integral part of the curriculum, and it was examinable.
- medical education
- humanities
- evaluation
Statistics from Altmetric.com
Author's note
In this paper I shall not draw any distinction between “arts” and “humanities”, although for other purposes it may be important to distinguish them. I shall use the term “humanities” throughout to mean subjects such as literature, history and philosophy.
1. Context
The establishment of this new journal comes at the same time as other major developments in the arts in health. A number of universities in the United Kingdom are now employing lecturers in the medical humanities1 and a new Centre for the Arts and Humanities in Health and Medicine (CAHHM) has been set up at the University of Durham. The centre will be involved in all aspects of the arts in health but there will be a major emphasis on medical education and on the evaluation of educational activities involving the arts. It is important that these developments are supported by reasoned argument and, where possible, evidence of effectiveness. This paper puts forward a number of arguments to justify the use of the arts and humanities in terms of the educational outcomes for future doctors; and then compares three educational structures in which the humanities were taught to medical students.
Before we discuss these, however, it is important to clarify the context—that of medical education which aims at producing the “good doctor”. What are the attributes of the good doctor? These are summarised in figure 1. It is clear that doctors need to understand their patients through a scientific knowledge of how the body works and to appreciate how scientific research can help them to make decisions about the best treatment for their patients. But this scientific approach needs to be modified in the clinical situation when dealing with the individual patient. A “humane” doctor is required, with the understanding, assisted by interpretative ability and insight, and governed by ethical sensitivity, to apply this scientific evidence and skills to the individual patient.2 The good doctor must also develop a sensitivity in her dealings with patients which is based on a knowledge of herself and her own values and imaginative insight into the problems and contexts of patients' lives. Doctors need then to be able to assimilate the scientific knowledge of disease and treatments with the understanding of the individual patient and to exercise good clinical judgment as to what might be of benefit to this patient with this particular problem at this point in his life.
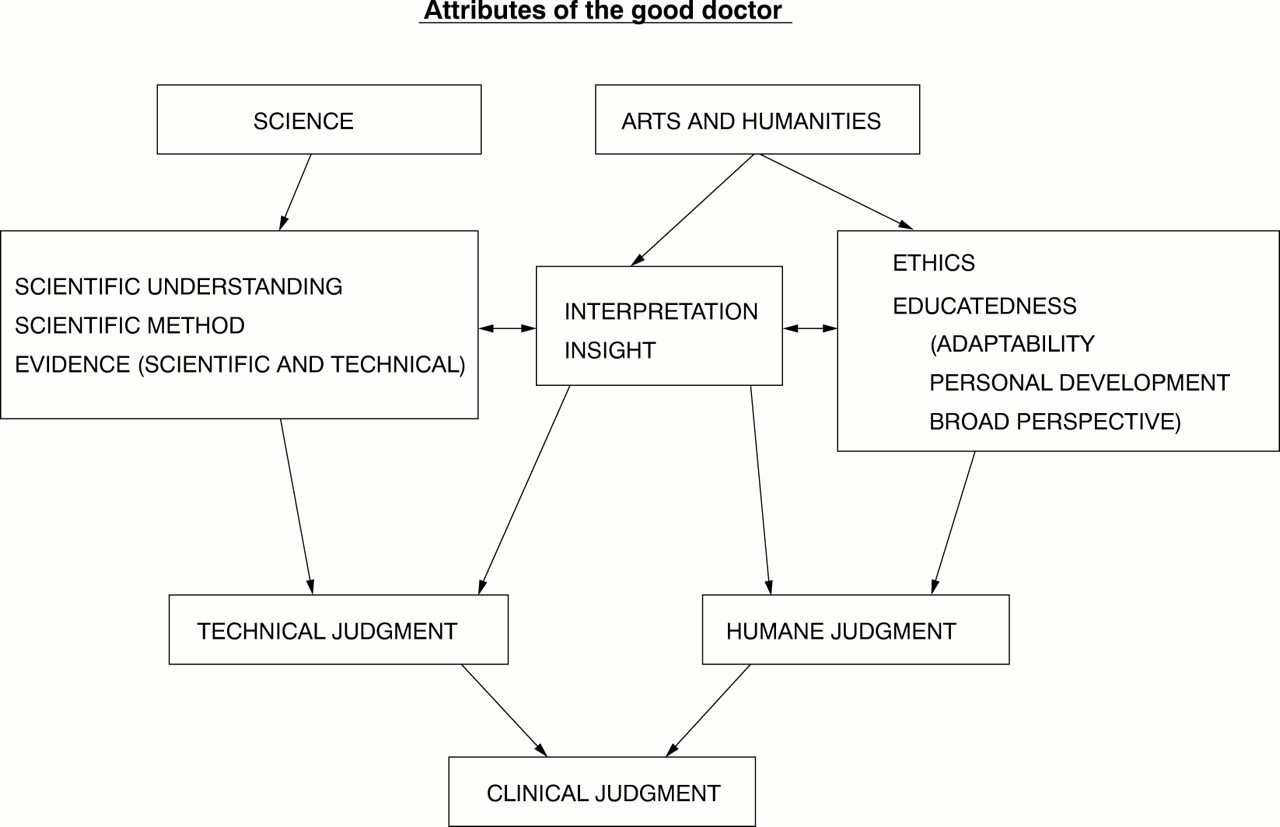
{kind=link}
This is a tall order for medical education to take on. In the last century the focus was largely on giving students the scientific knowledge and skills required of a doctor, but this is not enough. In 1993 The General Medical Council (GMC) recognised that medical education needed a radical rethink, and in their document, Tomorrow's Doctors,3 recommended a greater focus on education, as opposed to training, in the undergraduate degree. The good doctor, as the GMC suggest, must be an educated doctor and this is one of the major areas where arts and humanities subjects might make a contribution.4 It is in this context that this paper is written.
2.The role of the humanities in medical education: educational outcomes
There are two main ways in which humanities subjects might be relevant to medicine. One, often discussed, is that the humanities play a primarily instrumental role in the education of future doctors.5 Works of literature in particular may help to introduce students to problematic life situations with which they may be unfamiliar. Imaginative identification with the characters involved will allow them at least vicarious experience of these problems before having to deal with them as doctors in a clinical situation. Students may also learn useful skills from the humanities, such as what makes for good—and poor—oral communication, from drama; or the skill of analysis and argument (as we shall later see) from philosophy. But it would be to devalue the arts and the humanities to suggest that they should be seen merely as a means to an end, even in the context of professional or vocational education.6 Art, literature, drama and music, in all their many forms, are expressions of human creativity; they reflect human joy and sorrow, and human celebration and reflection. Part of what it is to be a complete human being is to participate in some form of artistic activity, either as spectator, reader or viewer. Understanding this will help doctors to remember the purpose of their own art: to enable people to participate fully in life unhampered as far as is possible by illness or disability. The humanities, therefore, have a second, non-instrumental role in the education of doctors. They do not merely have a usefulness in contributing to the development of ends other than themselves: they also have an intrinsic value in their own right and as such are essential components of the educated mind. As Downie puts it, “along with an understanding of the sciences they constitute what it means to be ‘educated’ as distinct from simply ‘trained’”.4
There is not, of course, a straightforward distinction between the instrumental and the non-instrumental uses of the humanities. For example, I have suggested that the understanding of the human condition which may come from literature is an instrumental use, but it is also part of a general educative process aimed at understanding more of life and how individuals respond to it. For the sake of clarity, however, and despite the overlap, I will continue to discuss the role of the humanities under these two headings.
INSTRUMENTAL USES OF THE HUMANITIES
Instrumental uses can be divided into two groups: humanities subjects, particularly literature, can be seen as a source of case histories for medical students; and the humanities can teach students certain skills which may be of benefit to them in the clinical situation.
Firstly, literature abounds with depictions of subjects relevant to medicine. The experience of depression is graphically portrayed in The Trick is to Keep Breathing, by Janice Galloway,7and in The Bell Jar, by Sylvia Plath8; and the poems “Ambulances” and “The Building”, by Philip Larkin9 describe what it is like to be a patient. Death and the experience of bereavement are frequent topics for writers such as Douglas Dunn in Elegies,10and C S Lewis in A Grief Observed.11 The advantage of studying works of literature rather than case studies of real patients is that through the skill of the writer our imaginations are stimulated and our sympathies aroused: the writer gets us involved with the characters so that we experience their trials with them.12 Anne Scott has explored the idea of the development of the “moral imagination” in health care workers and has suggested that the study of literature may help to develop practitioners who are (in the words of Henry James) “finely aware and richly responsible”.13 By getting us involved with the characters, good literature can make students “finely aware”—a non-instrumental value in our context. But for literature to have an instrumental use we must take a further step if we are to encourage students to consider how they would respond if they were to come across people with similar problems in professional practice, and to have responsibility for their care. This further step requires that students be directly challenged to consider their hypothetical responses to the fictional character or situation. This can be done in group-work sessions and if the students' imaginations and feelings are engaged, then the discussion will expose hidden prejudices and fears and allow discussion of the issues in a “safe” environment.
Secondly, how can literature and the humanities more generally teach useful skills which may be transferable to the medical context? Literature can teach about written communication, but, more importantly for health care, drama demonstrates the nuances of communication between people, both verbal and non-verbal. Indeed, most communication skills courses now involve role play for the students with actors playing a part. Painting may also bring out the non-verbal ways in which feelings or attitudes can be expressed. The well-known painting “The Doctor”, by Sir Luke Fildes illustrates eloquently the nature of the doctor-patient relationship.4 The doctor leans over his patient, a sick child, with a look of deep concentration in his face. The light in the picture focuses concern on these central characters while the parents stand, almost unnoticed, in the background.
History and philosophy may also train the students in useful skills. History can teach the importance of evidence and how it can be manipulated by individuals to give a fraudulent view of the truth. The medical world has become increasingly aware of fraud in medical research recently14 and students may find it easier to understand the principles of how evidence can be interpreted in different ways in a historical context. More specifically, the study of the history of medicine can remind students of the transient nature of much medical knowledge and of the importance of keeping up to date with developments. Philosophy (which is also important in the non-instrumental context) can teach students to order their thoughts, construct an argument and reach a logical conclusion. These skills are essential in diagnosis, where the doctor must gather information to support a thesis and go through logical steps to reach a conclusion. I will illustrate this use of the humanities in the discussion of the philosophy module in the last part of this paper.
NON-INSTRUMENTAL VALUE OF THE HUMANITIES
Turning now to the non-instrumental value of the humanities, I wish to argue that that value has three aspects: in education, and relatedly in personal development, and in providing the opportunity for students to step outside the pervasive ethos of the medical world and experience a kind of “counter culture”.
Turning first to the educational point, we can say that medicine is regarded as a “vocational” qualification at university in that it prepares the students for a particular job at the end of their degree. We talk of students being “trained” to be doctors, rather than being “educated” in medicine. It is important in this context to be aware of the distinctions between education and training, and I will draw here on the work of the educational theorist R S Peters.15 In a medical context, similar distinctions are drawn by Calman and Downie.16 Briefly, to be educated is to have a broad perspective, as distinct from the narrow focus of training. Secondly, education is a process, not a single objective. As Peters says:
“to be educated is not to have arrived; it is to travel with a different view”.17
Peters's final point is that an educational process should be valuable as an end in itself and not just because it enables someone to do something else. When we speak of training the questions asked are to be trained “in what” or trained to do what? But these questions do not fit the educational process.
These points were clearly in the minds of the GMC when they wrote Tomorrow's Doctors. Commenting on the deficiencies of current undergraduate medical education they said that the current system resulted in a
“regrettable tendency to underprovide those components of the course that are truly educational, that pertain to the proper function of a university and that are the hallmark of scholarship”.3
Clearly, the education of future doctors will involve some training as well as some educational activities and the GMC here pointed out that the latter have tended to be neglected. By allowing the study of literature, history or philosophy in the medical curriculum, we shall at the very least introduce breadth. But, more importantly, these subjects can challenge the students by introducing them to some of the great thinkers and will allow them to consider different ways of perceiving the world. This will encourage a critical and questioning attitude and help develop judgment.
Turning, secondly, to the value of the humanities in personal development, we can say that the educational process touches the student more deeply at a personal level than does the training process. Education is not just concerned with what someone can do, but about what kind of people they become as a result of their education. Developing as a certain kind of person is important for the good doctor because medical practice is not just concerned with knowledge and skills but is also concerned with a humane and sympathetic approach to people. This is a quote from the essay “On Liberty” by JS Mill:
“It really is of importance, not only what men do, but also what manner of men they are that do it. Among the works of men, which human life is rightly involved in perfecting and beautifying, the first of importance is man himself”.18
It is here that a study of literature is best justified. As I have suggested, plays, poems and novels demand an emotional response from their readers and in doing so they will allow the students to discover their own hidden values and prejudices, and to challenge them. This will encourage the kind of self understanding (“fine awareness”) which is essential for the development of mature human beings who are attuned and sympathetic to the perspectives and values of other people.
The final point about the non-instrumental value of the humanities is their role in providing the experience of a “counter culture” to medicine. Medical students often have the impression, and are encouraged in it by medical teachers, that they have an intellectual and moral superiority over other students. This is not helped by the fact that entrance requirements for medicine are amongst the highest in the university system or that medical students' university experience tends to be rather insular, in that everyone follows the same course. The opportunity to take a humanities subject will allow medical students to meet teachers and students in other disciplines, will help reduce this isolation and may ultimately foster better relationships between doctors and the “outside world”.
The GMC have now provided an opportunity for students to take advantage of what the humanities have to offer within the structure of the curriculum. In their desire to increase the educational content of medical degrees, the GMC have suggested that arts and humanities subjects may be offered to students as part of their course in the form of “special study modules”.19 These SSMs are to take up as much as one third of the total course and should be four-five week blocks set aside from the rest of the course to “allow the students to study in depth areas of particular interest to them”.3 I will shortly discuss one such module, which has been piloted in Glasgow, but as a comparison I shall first evaluate two other humanities courses.
3. Structures: a comparison of the three courses
VOLUNTARY COURSE
In 1985, I was amongst a group of students who were involved in a voluntary course for 3rd year medical students which met in the evenings of the summer term. The course was run by a number of interested teachers in the medical faculty, including a general practitioner, a philosopher and the postgraduate dean. The aims of the course were to introduce the students to literature in its broadest sense, so they could learn about life by reading of the views, insights and feelings of others, and to encourage them to examine their own attitudes and prejudices.20 We read poems and extracts from medically relevant literature and discussed them in groups with the tutors. The evaluation suggested that 80% of the students felt the course aims had been met. Students' reasons for attending included: “I came to broaden my views” and “to try to stay human as well as being a doctor”. They were keen that the course be run again, as long as it remained voluntary.
This course was very successful and popular with the students, but attendance was sporadic and it felt more like a club for interested people than something integral to the students' education as doctors. Despite the involvement of the postgraduate dean for education (who left the university soon after the course was finished), the course did not run for a second year, as there was neither financial nor moral support for it amongst other members of the faculty. The group has, however, continued outwith the university and is still running, over 14 years later. It now consists of practising doctors from different specialties, dentists, philosophers, and interested others. We meet two to three times a term to discuss a book, poems, a play or film we might have seen. The discussion ranges widely but often touches on how these works might have helped those of us who are clinicians. The involvement of people who are not clinicians is extremely helpful in clarifying the patient's perspective.
The seed planted by this voluntary course flourished quickly and it was greeted with excitement and enthusiasm by both students and teachers. It continues to flourish as a voluntary club but it did not become established as a part of the medical curriculum in any form because support was not there to sustain it. Students attended and enjoyed the group but they did not regard it as a central part of their education.
COMPULSORY FINAL YEAR SESSION
From October to February 1997/8 I attempted an experimental course with the final year students in general practice. In a 90-minute session they were introduced to the idea of medicine and literature and were given reasons why broader reading might help them in their education. They were then split up into groups and set to read a passage from The Trick is to Keep Breathing, a novel by the contemporary Scottish writer, Janice Galloway, which gives an account of the experience of depression. Some groups discussed three contrasting poems on old age, including the humorous poem by Jenny Joseph, Warning.21 In the groups the students were asked to discuss some questions such as: “How might these poems help us to understand our elderly patients?”
Some groups (the minority) took the whole exercise very seriously and really got into the idea and became quite animated; for a few, their excitement derived from the fact that they could recognise a patient they had seen in what they were reading. But the evaluation showed that although the students' interest had been aroused (and, from what I observed in the groups, they had made a connection between the material and their clinical work) they did not rate the course very highly in terms of usefulness to them. Here are some of the comments students made: “Some [of us] just read the back page of the Sun, which is fine cos we are all different”; “woolly”; “less of the literature: not very useful”.
This course differed from the first in that it was compulsory. Perhaps because of the compulsion, it was less successful than the voluntary course. The comments and the poor rating for usefulness reveal an attitude that is a problem in vocational courses such as medicine: the students tend to regard as important only those classes which they see as being directly relevant to the job of being a doctor. Medical students have traditionally looked down on subjects such as psychology or sociology, which they see as being at best common sense and at worst unimportant to their future clinical work. This problem may be compounded with subjects such as literature and philosophy, which have even less obvious relevance to them. The moral of this type of structure is that it will be impossible to interest all medical students in the humanities as part of their medical education, even if we feel that it would be of benefit to them all. If students are to respond they have to be open to, and interested in, what they are reading. If they read literature or philosophy on sufferance it will be of no value to them at all.
In this course the seed scattered by the humanities fell largely on stony ground. I can only speculate that for some of the majority who did not respond well to what they had read, a shoot might stir in the future when they see a depressed or elderly patient. They might then begin to understand the relevance to them of the insights of literature.
From these first two examples, we can derive two structural conditions for courses in humanities in medical education. Firstly, they should be freely chosen options; and secondly, they should have some integrity as part of the medical degree. With the advent of the new structure in undergraduate medical education—of “core” and special study modules (SSMs)—it is now possible for humanities courses to satisfy both conditions. Moreover, the new structure permits, indeed requires, a third condition, and for medical students this may be the most important of the conditions for a successful course: the SSM must in some way be examinable. The final course I will describe had the advantage of all three of these conditions: the students were self selecting, but the course was also, as an SSM, regarded by them as part of their degree, and they had to achieve a pass in it.
SPECIAL STUDY MODULE IN PHILOSOPHY
February 1998 was the first time SSMs had been run in Glasgow and the students were offered a module in philosophy entitled “the individual in society; an introduction to social and political philosophy”.22 This module was the product of a collaboration between the departments of general practice and philosophy and enabled the medical students to take part in a course which was being taught to first year students of philosophy. I will describe the course—its aims, structure and assessment—and go on to show how the three main aims are related to the education of doctors. The question of whether the course succeeded in its long term purpose of broadening the outlook of future doctors cannot yet be answered, but I will describe the initial evaluation by the first group of students and their assessment of whether the course was valuable for them.
The course had three main aims:
-
To read and discuss Plato's Republic;
-
To encourage the students to adopt the techniques of philosophical analysis in their approach to an argument, and
-
To expose them to the broadening experience of an academic culture different from their own.
The module provided ten second year medical students with the opportunity to spend five weeks studying Plato's Republic in the context of a course of lectures on political philosophy. As offered in Glasgow, special study modules have the advantage that they are five-week blocks set aside from the rest of the course, during which students can concentrate solely on their module subjects. The medical students were, therefore, able to fit in with a pre-existing course on political philosophy which was about to start at the same time as their module. The lectures and reading material from this course became part of the module. Our medical students were therefore partly taught alongside the arts faculty students and were taught by philosophers who were not specially angling their material at a medical audience—an important point in terms of the third aim, that of exposing the students to a different academic culture.
What is the justification of the three aims in the context of medical education? Of what benefit is five weeks of philosophy to medical students, and why should they learn about Plato?
The justification of the first aim is that The Republic deals with fundamental issues relating to society, such as the reasons why people live together in communities in the first place. Humans are frail beings and need the protection of a group, and there is a need to share human resources in the form of the diverse range of talents that people have. Without reference to religious morality, Plato deals with the moral values which, of necessity, must rule human society, granted these human needs and vulnerabilities. This approach opened the students' minds to a deeper understanding of the origins of our society's make-up and of the values which allow it to function. From this point of view the module had a non-instrumental educational value. As it happened, the students had just completed their family project in the medical course, so they were challenged by Plato's rejection of the family as the basic social unit. This was an unexpected educational bonus.
The justification of the second aim is in terms of its use in developing transferable skills and attitudes. Clinical diagnosis requires that doctors be able to sort out information about a patient, order it and construct arguments for or against certain conclusions (diagnoses). Philosophy can teach students how to go about this; a major part of the module focused on learning about argument, and students were taught the steps to take in constructing arguments. Besides learning how to do this for themselves, the students also learned to recognise when others were making arguments and when these arguments might be valid or invalid. This was a particular revelation to them (as I will show in the evaluation) as they had been used to accepting much of what they were told. Most of the students commented that by the end of the module, they had begun to question received wisdom with much more confidence.
The justification of the third aim is that it distanced the students from the pervading culture of their medical education and medical class and placed them in the arts faculty (physically and intellectually) and amongst philosophy students and teachers. This provided a broadening academic experience, a “counter culture”, and one that the students would recognise and value as different.
From the practical point of view placing the medical students in an arts faculty context was also a help. It was fortunate that there was a course on political philosophy going on in the philosophy department at the same time which enabled us to do this. This “piggy backing” idea helped us to overcome the problem of getting arts teachers involved in the course. Other solutions might include joint teaching between the faculties and getting colleagues from other departments interested in teaching the medical students. However, in the current climate in universities, it is important that structures are devised to give collaborating departments equal credit for participating in such courses.
There were three parts to the assessment of the module. For the class essay, consisting of 70% of the marks, students were given a choice of two titles: “Do we have a moral obligation to obey the laws of the state?” and, “To what extent can one justify the criticisms of democracy which Plato makes in The Republic”? Students also had to complete two seminar papers, contributing a total of 20% of the marks, and two analytical exercises contributed the final ten per cent. One analytical exercise was handed out at the start of the module and one at the end, to see how their analytical skills had progressed. The exercises consisted of two paragraphs of contrasting arguments, the first relating to lie-telling and the second, to the relative moral value of doing voluntary work out of a sense of duty or for enjoyment. The students were asked to identify the arguments and suggest whether they were valid or invalid.
Evaluation was carried out in two ways, firstly, by a conventional questionnaire, which asked the students about their reasons for taking the module and what they thought of the structure, content and educational value of the module; and secondly, by comparing the two analytical exercises that the students did at the beginning and end of the module, to see how their analytical skills had progressed. These results relate to our 1998 group of ten students.
In their responses to the questionnaire most of the students said they had taken the module because they were keen to do an arts subject again, having missed the opportunity to study the arts since leaving school, and nine out of the ten wanted a complete change from medicine. Again nine out of the ten students felt stimulated by the discussion in seminars and by the new ideas that were introduced. They were keen for more discussion time and for more time spent on clarifying issues they did not understand from their reading and lectures. The group seemed to have handled the content of the module well and most felt that they were better able to analyse argument by the end of the course. Most (seven out of ten) also said that they would be able to describe the major arguments of The Republic to a friend.
In the second half of the questionnaire, the students were asked about their views of the educational value of the module for themselves. All had discussed the module with their colleagues, indicating that the students had become interested and engaged in what they were doing (an important prerequisite for an educational activity). Most of them, indeed, wanted to do more philosophy in the future and had ideas they wished to pursue. We asked them specifically about the value of the module in medical educational terms and the most frequent comment here was that they would now be less inclined to accept things they were told without justification and they would be more critical of what they were told.
The second part of the evaluation involved a comparison of the first and second analytical exercises as a more objective measure of whether the students had succeeded in learning the skills of analysis. In the first exercise, the students were unable to identify specific arguments and they had no idea of what constituted validity. Most of the analysis consisted of whether they agreed or disagreed with the arguments presented. By the end of the module, six out of ten of the students had reached quite a high level. They were able to list the arguments used in the passages, and outline their logical sense, separating premises from conclusions. All of the students attempted to analyse the arguments for validity and most succeeded.
This module was designed to broaden both the students' education and their views of society and its structures—a non-instrumental role for the humanities. The process by which it helped them to do this enabled them to learn the technique of philosophical argument and how to apply it themselves—an instrumental role. The initial evaluation would imply that the seed we have planted has taken root but it will be a rather longer term exercise to prove that it will flourish and will make any difference to these young people in the future.
4.Conclusion
Arts and humanities subjects (and in this paper I have focused on literature and philosophy) may be valuable in medical education but not all medical students respond enthusiastically to this teaching. There are three possible responses—and here the metaphor of seed planting is relevant. Firstly, (as with the literature group and philosophy module) some students will fall upon the opportunities offered by studying literature and philosophy with delight and it will produce an immediate flowering of the imagination and the understanding. Secondly, many students, such as the final year class, will be left cold until, perhaps, an encounter with an individual patient germinates one of the seeds we have planted, as they remember something they have read and discussed, which enhances their understanding of their patient's problem. Thirdly, some students, perhaps the majority, will never see the value of the broader educational base and skills that arts and humanities subjects can bring to them—and there is nothing wrong with this as medicine is a discipline which requires many different sorts of people.
It is clear that the students need both the freedom to choose to take up the opportunity of broadening their educational experience by taking humanities subjects, and the impetus to work that comes from these subjects being an examinable part of the curriculum. We are fortunate in the undergraduate arena that we have the SSM structure which allows humanities subjects to be introduced for students who wish to take them. We can also make use of skills and ideas from philosophy, history and literature to illustrate and illuminate teaching in other areas of medical education—such as in communication skills and behavioural science—and thus suggest their instrumental value to all medical students. Medical practice consists of a wide range of different jobs requiring many different sorts of people and the educational benefits of the humanities may not be appropriate for them all. We must avoid expecting an enthusiastic response from all medical students.
Footnotes
-
Jane Macnaughton, MA, MBChB, MRCGP, PhD, is Director of the Centre for Arts and Humanities in Health and Medicine (CAHHM), University of Durham, Business School, Mill Hill Lane, Durham, DH1 3LB.