Article Text

Abstract
The recent policy focus in British public health on the importance of local action invites consideration of historical precedent. The role and achievements of the medical officer of health (MOH), the local government official charged with public health responsibilities, is discussed. The gradual accretion of duties is traced in the first section: the mid-Victorian concern with urban sanitation; the preventive strategies adopted after the bacteriological revolution; the extension of personal health services in the early 20th century; and the more diminished role under the National Health Service (NHS), when infectious diseases retreated. The historical verdicts passed on the MOsH are reviewed in the second section. The leading role of the MOsH in the late 19th-century mortality decline has been reasserted, and although there is some justification in the argument that in the 20th century public health lost its focus, it is important to recall that the extension of personal health services under MOH direction signified a major extension of access to care. Similarly, the charge that MOsH did not redefine their role in the period before their final demise in 1974 is not entirely justified. The emphasis of the NHS on curative rather than preventive medicine, and the economic constraints on local authority health service expansion limited their room for manoeuvre. The history of local leadership in public health may offer some enduring lessons. These include the importance of monitoring local population health, acting as a public interface between medicine and the community, facilitating joined-up working and confronting vested interests.
- GP, general practitioner
- MOH, medical officer of health
- NHS, National Health Service
- TB, tuberculosis
Statistics from Altmetric.com
Since the 1980s, an important feature of public health, internationally, is an emphasis on the local, rather than the national, as the arena of action. For example, the Ottawa Charter in 1986 called for the empowerment of communities as a key strategy for meeting the World Health Organization’s Health for All goals,1 whereas the World Health Organization’s Healthy Cities initiative was targeted at the urban level.2 In Britain too, the reinvigoration of local initiative has been central to the recent review of public health policy. This partly seeks to mobilise individuals, private enterprises and voluntary organisations, but it also recognises that a strong corps of health workers within the public sector must take the lead if local initiative is to succeed.3–5 From the vantage point of history, there is a certain irony in this rediscovery of the local. After all, it was through the medium of urban local authorities that the British state pioneered its mid-19th century programme of sanitary reform, a template for attacking infectious diseases which was adopted by other industrialised nations.6 When considering the status of public health in Britain over the long term, it is arguable that under the National Health Service (NHS) the experience has been one of decline and fall from an earlier golden age of locally driven action.7,8
The subject of this article is the medical officer of health (MOH), the official who led the amply staffed public health departments once situated in local government. This post was abolished in the 1974 health service reorganisation, when MOsH were superseded by community physicians within the NHS and local government health services subsumed in Social Services Departments. Now that preventive medicine and health promotion are firmly back on the local political agenda, and the profile of the specialty raised through the appointment of Directors of Public Health, what can we learn from considering this history? The first section describes the development of the MOH’s role since its inception until 1974. The second part discusses historical appraisals of the MOH and the final section points to several areas of this experience, with implications for today’s local leadership in public health.
RISE AND FALL OF THE MOH
1872–1914
The idea of a medical appointee who would give direction to local authorities originated in Edwin Chadwick’s report on the Sanitary condition of the working population of Great Britain (1842). The first such posts were held by William Henry Duncan in Liverpool and John Simon in the City of London, although these appointments become mandatory only with the Public Health Act of 1872.9 This positioning of public health within local government may seem inevitable in retrospect, so familiar is the story of sanitary reform in the burgeoning industrial cities. Yet, it also indicated the dominance of the Chadwickian faith in environmental cleansing. Miasmatic theory was not the only method available to explain the cause of disease, but, in the heyday of laissez-faire capitalism, programmes on sewerage and fresh water were a technical fix that suited policy makers better than more radical options such as income redistribution or social housing.10 A key concern of the early MOH was therefore the physical environment, but various other duties developed, indicating the medicalisation of public health that began during the tenure of John Simon as the country’s first Chief Medical Officer. One was the preparation of an annual report on the sanitary state of his district, and in these texts the beginnings of epidemiological reporting may be traced.11 Crude death rates, cause of death tables and infant mortality became standard features, and from the 1890s, some introduced adjusted-death rates and the incidence of legally notifiable infectious diseases, such as cholera, diphtheria, typhoid and scarlet fever.12 With the infrastructure of sanitation being put in place, the remit of public health extended to tackle infectious diseases through the establishment of isolation hospitals and the appointment of specialist officers under the MOH’s control. The Pasteurian revolution added bacteriology to the MOH’s toolkit, and by the 1910s, laboratory facilities were provided either by a public analyst or under contract from universities or hospitals. These underpinned preventive and curative services for infectious disease and enabled MOsH to enforce food safety legislation. Finally, the late Victorian government promoted slum clearance and housing improvement schemes, with the MOH and local sanitary committee as prime movers in such initiatives.
1918–1948
The apogee of MOH power was in the first half of the 20th century. They oversaw state welfare programmes to improve the health of mothers and children, channelled through local government and partly inspired by imperialist and eugenicist concerns.13 A school medical service was set up and it was usual for the MOH to also be the area’s school medical officer, with responsibility for inspections and treatment.14 Antenatal and infant welfare clinics were established, maternity hospital beds increased, health visitors employed and certification of midwives was introduced. Partial state funding also supported local authority initiatives against tuberculosis (TB) and sexually transmitted diseases. Before the BCG vaccine, TB policy consisted of notification by general practitioners (GPs), public provision of municipal clinics and sanatoria, and voluntary sector contracting for hospital beds and rehabilitation schemes, all coordinated by the MOH. The association between TB and domestic overcrowding meant a continuing role for health within the housing policy, following legislation that promoted slum clearance and council house building. Environmental duties of the MOH extended to encompass pest control, food safety (fig 1), provision of public conveniences and sanitary controls in port cities. Also, following the Local Government Acts of 1929, municipal authorities could take control of the old Poor Law workhouses, many of which already functioned as chronic disease hospitals. The policy aim was to remove the stigma of pauperdom and usher in publicly funded general hospitals under MOH control. These could augment voluntary bed capacity and knit institutional provision into the larger framework of local health policy.15

Health slogan lantern slide, Central Council for Health Education, 1929. Reproduced with the kind permission of the Wellcome Library, London. This example of “health propaganda” from the interwar period illustrates the beginnings of health promotion and the crusade for food safety, and also the ideal of the medical officer of health as a local figurehead for public health.
Wartime brought additional challenges as MOsH struggled to deal with the health impacts of aerial bombing, mobilisation, and a drastic reduction in civilian hospital beds. However, optimism prevailed about the future, particularly when the coalition government’s white paper of 1944 proposed a national health service based on local government.16
1948–1974
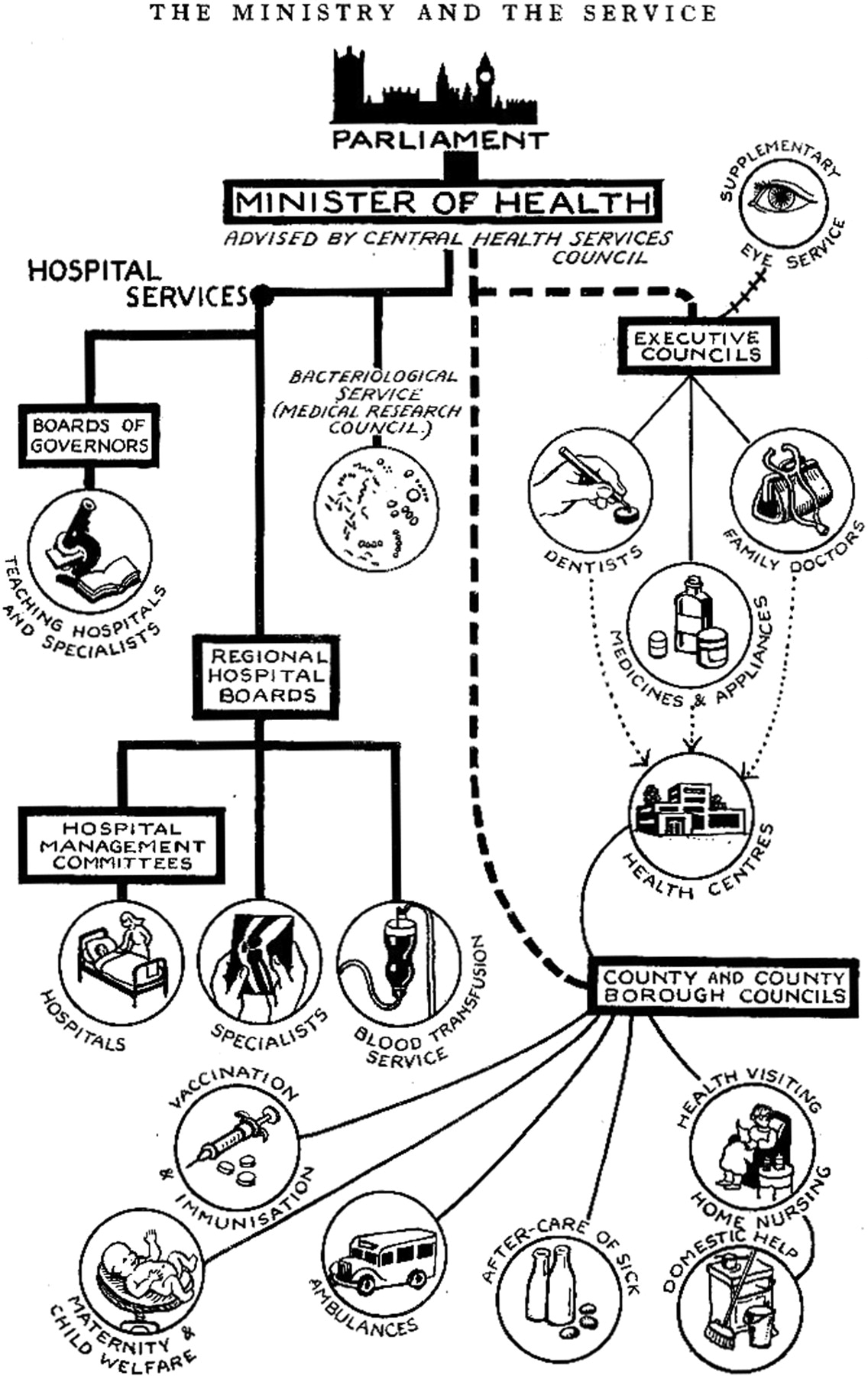
In the event, vested interests prevailed over the planners’ ideals. To secure the agreement of the British Medical Association for the NHS, Aneurin Bevan conceded that the administrative structure of the hospital service should be distinct from that of local government. Municipal hospitals and sanatoria now fell under the remit of the new regional hospital boards, dominated not by MOsH but by the academics, business people and consultants who had hitherto run the voluntary hospitals.17 What remained was the responsibility for vaccination and immunisation (directed initially at diphtheria and whooping cough), the ambulance service, and maternity and child welfare, with the associated activities of health visiting, domiciliary nursing and home help (fig 2). Staffing of public health departments contracted with the loss of municipal hospitals, although an urban MOH’s team in the mid-1960s might have contained officers responsible for school health, maternal and child health, occupational health, epidemiology, the ambulance service, nutrition, health education and medical social work, and a team of sanitary inspectors to carry out environmental health duties.18 These included maintenance of sewers, assuring water purity, housing policy, milk and meat inspection and pest control, along with a new focus on noise and air pollution, particularly after the Clean Air Act of 1956.

{kind=link}
{kind=link}
The organisation of the National Health Service. Reproduced from The Practitioner, extra number, The National Health Service Act in Great Britain, Autumn 1949, p 79, by kind permission of the publisher.
The break-up of these empires came in the 1970s, when the MOH’s duties were divided between different agencies. Separate social services departments were created in 1971, with responsibilities of home help, domiciliary nursing and the welfare of elderly people, mothers and children. Then, in the 1974 NHS reorganisation, health visitors were attached to GP surgeries and the new post of community physician was created, part epidemiologist and advisor, and part manager of local authority health services.19 Environmental health remained within the local authorities, though with some loss of authority.19 Although some existing MOsH became community physicians fewer such posts were available, and for some the position was of lower status.20,21 For public health, the reorganisation was, in the words of Sir Donald Acheson, “the disaster” (Berridge et al,8 p 18).
HISTORIANS AND THE MOH
Historical verdicts on the achievements of the MOH have been far from unanimous. For the 19th century, a fierce debate has raged about the relative importance of preventive medicine in the decline in British mortality, triggered by Thomas McKeown’s well-known thesis. This dismissed the significance of health services and medical science in conquering infectious disease, which McKeown22 attributed instead to improved nutritional status. Public health measures were acknowledged to have played a lesser part, limited to the control of water and foodborne diseases. Subsequent exchanges questioned some aspects of McKeown’s methodology and interrogated the association between the timing of decline in mortality and rising living standards.23 Broadly, this work reinstated the importance of local government public health interventions. Meanwhile, microhistories of local programmes against diseases such as smallpox, typhus, typhoid and TB have shown how the Victorian preventive administration was instrumental in bringing down mortality.24
Criticism of performance of MOsH in the first half of the 20th century, turns on the claim that with their energies spread thinly across both environmental and personal health services, the focus of public health work was lost.20,25 One example is the failure to apply advances in nutritional science to school medical work, so that child malnutrition went under-reported, particularly in areas hard hit by interwar depression.26 Another failure was the slow adoption of diphtheria immunisation strategies, despite evidence of their success in North America.27 Again, studies of individual locales have shown that some progressive MOsH did move forward in these areas,28–30 and it should also be stressed that national leadership from the Ministry of Health and the Chief Medical Officer was lacking—a reflection of official caution and conservatism.31 On the credit side, the personal health services under the MOH’s control saw some expansion in the 1920s and 1930s, despite a general atmosphere of resource constraint.32 Above all, greater equity was introduced to the health system by broadening access to care. This was achieved through the removal of the stigma of the Poor Law from publicly funded medicine, thus, opening up maternity and general hospital care to those with lower incomes by right of citizenship. By its nature localism was uneven, and some MOsH were constrained by ratepayer parsimony or residual adherence to the Poor Law tradition. Nonetheless, with 57 318 beds in English and Welsh municipal general hospitals by 1938, many for acute care, progress to more equitable provision was underway well before the NHS. Finally, interwar MOsH were instrumental in encouraging public housing programmes. As the MOH for Bath observed in 1920, when imploring his council to enforce closure orders and commence constructing new buildings: “Of all the causes which tend to undermine the health of the people, a shortage of suitable housing accommodation is by far the greatest.”33
The charge against MOsH in the early years of the NHS is that they were, in some respects, authors of their own downfall. One problem was their failure to redefine the role of preventive medicine now that the threat of infectious diseases was receding. It was not until the 1970s that the new public health emerged, with its focus on the risks of cancers and cardiovascular diseases and on individual lifestyle.34 Another difficulty was the apparent divorce between the practice of MOsH and academic public health. Here a key influence was John Ryle, who urged that the discipline be reformulated more broadly as social medicine, which foregrounded epidemiology, placed a new focus on chronic disease and took a more holistic view of the social causes of ill health.35 The public health leadership, represented by the Society of Medical Officers of Health, was unenthusiastic about this turn, but did not articulate an alternative vision of its purpose, leaving it vulnerable when social services departments challenged its terrain.20
Once again, local studies are moderating this picture by showing that reorientation was underway, with various new initiatives in the fields of health education and screening programmes.36,37 Indeed, early ventures in smoking cessation were tried, but were poorly supported, before the government raised the profile of lung cancer risk through fiscal policy and advertising restrictions.18,38 MOsH were also the victims of trends in general practice and social work. When the NHS was planned, Bevan envisaged a network of health centres that would integrate GP and local authority services (fig 2), including health visitors, child welfare, antenatal classes and health education. However, few were opened, owing to both cost concerns and lingering fears that they might transform doctors into state employees.39 In addition, the scope given to MOsH to develop community nursing and health visiting for elderly patients and those with mental illness was circumscribed by lack of resources. Pressures also came from GPs themselves wishing to take greater responsibility for community services, and by the 1960s experiments in health visitor attachments to GP practices were underway.20,37
Meanwhile, the profile of social work was rising. Hitherto, social services had been divided between local education, welfare, health and children’s committees, but a momentum for reform builtup as generic training courses were developed and a professional association was formed.40 This culminated in the Seebohm Report (1968), which recommended the establishment of unitary social services departments by local authorities to draw together all their social workers, thereby depriving MOsH of much responsibility.
In summary, the failure of the post-war MOsH was not entirely of their own making. The orientation of the NHS towards the hospital service and the attenuation of local authority powers had marginalised public health, demoralised the profession and deprived it of resources. Moreover, the claims of social services were legitimate and bore fruit as funds for social work rose. By the early 1970s then, a new conception of public health was emerging distinct from the existing activities of the profession. While the MOH’s successor, the community physician, was drawn into administrative work for health services, the focus of public health action moved elsewhere, for example, into new activist bodies such as Action on Smoking and Health, founded in 1971 to combat smoking. Yet, soon after 1974, fears that something had been lost with the MOH began to be articulated.
ANY LESSONS FROM HISTORY?
What can this exercise in recalling the role of the MOH tell us about local leadership in public health? One overarching point is that MOsH enjoyed securely tenured appointments, independent of the committees that managed services. This gave them scope to operate as autonomous advocates for people’s health.
There were several aspects to this. One essential duty whose value has been rediscovered was the annual report on local population health. Although mindful of their earlier weaknesses, the 1988 Acheson Report advocated this as a core activity of Directors of Public Health, as did the 2004 Wanless Report.4,7,41 Historically, the annual reports provided an empirical basis for claims on local government expenditure and permitted the monitoring of changing patterns of need. Indeed, it was recently noted that one reason why the incidence of sexually transmitted diseases has risen so dramatically since the 1980s was that: “nobody had actually thought about how we would keep an eye on them …” (Berridge et al,8 p 9). Such oversight also signified a clear chain of responsibility. Significantly, the Acheson Report into public health was triggered both by the HIV/AIDS crisis and by two food-poisoning scandals, which raised fears that with the MOH gone, the control of communicable diseases had been weakened.7
A high-profile local figurehead for public health also provided the interface between medicine and community. In the late 19th century, for example, the MOsH were credited with instilling notions of domestic hygiene and norms of healthy behaviour. Their campaigns of health education through print media, lectures and domestic visits were instrumental in dislodging traditions of domestic privacy and fatalism towards sickness, thus promoting acceptance of preventive medicine.24 Their interwar expansion of infant welfare and antenatal clinics provided another channel for education, and contributed to the improvement in maternal and child health.40,42 After 1948, the successful MOH was prepared to disseminate information and step into the media spotlight—for example, Robert Wofinden, MOH for Bristol, a champion of health centres, who issued monthly health bulletins to local GPs and regularly appeared in local press and television where he was “… the very embodiment of competence and uncommon sense: the personification of reassurance, trustworthiness and reconciliation.”43
Although such paternalistic attributes are perhaps out of tenor with expectations today, the requirements of networking skills and personal diplomacy are more enduring. The interwar MOH was a key figure in integrating municipal, Poor Law and voluntary sector services, not to mention negotiating with GPs suspicious of state medicine and local politicians keen to restrain taxation. Ministry of Health observers in the 1930s were clear that success depended on the abilities of MOsH to facilitate joined-up working: personal animus could frustrate the public good, whereas those able to build strong alliances could ensure “… the health orchestra rhythmic rather than syncopated may give forth harmony and not discord …”.44 Subsequent research into interdepartmental or cross-sectoral joined-up working confirms the importance of tactical actors with an appetite for politicking.45,46
Leadership also involved the preparedness to face down vested interests.47—for example, Arthur Newsholme, MOH for Brighton, who enforced meat safety over the complaints of the butchery trade and its political allies.12 Or John Parlane Kinloch, MOH for Aberdeen who pioneered the removal of public hospitals from the humiliating Poor Law, in defiance of local medical opinion, which held that only the voluntary sector should provide acute care.29 These examples suggest a final legacy of the MOH’s work: the ethical component of leadership in public health. To engage with disease as a social phenomenon was to confront the problems of health inequalities and equity of access. The requisite skill was to be sufficiently impartial to be authoritative, and yet at the same time, to advocate for the disadvantaged.19 At their best then, the MOsH embodied the aspiration that John Ryle laid down for social medicine in 1942: a combination of “social conscience as well as scientific intent”.48
What this paper adds
-
The recent policy focus on the importance of local action in British public health invites consideration of historical precedent.
-
This article examines the rise and fall of the medical officer of health (MOH), the local government official once responsible for public health duties in Britain.
-
It surveys the growth of local environmental, preventive and personal health services before the National Health Service and describes the curtailing of MOH’s responsibilities after 1948.
-
It points to several areas of historical debate over the contribution of the MOH to health improvement and concludes with reflections on the lessons to be drawn from this experience of leadership in public health.
-
At their best, the MOsH were independent actors who monitored local population health, functioned as a public interface between medicine and the community, facilitated joined-up working and confronted vested interests.
REFERENCES
Footnotes
-
Funding: This study is funded by a Wellcome Trust University Award.
-
Competing interests: None declared.
Linked Articles
- In this issue