Article Text

Abstract
Numerous medical schools have been updating and modernising their undergraduate curricula in response to the changing health needs of today’s society and the updated General Medical Council competencies required for qualification. The humanities are sometimes seen as a way of addressing both of these requirements. Medical humanities advocates would argue that the humanities have a vital role to play in undergraduate medical education, allowing students to develop the critical tools required by the 21st-century clinician to deliver the best person-centred care. While we endorse this view, we contend that such training must be taught authentically to have maximal impact. This article arises from a collaboration between Imperial College London and Birkbeck, University of London, which aimed to embed the humanities into Imperial’s undergraduate medical curriculum. Here, we use a teaching session on graphic medicine and narrative as a case study to illustrate how the humanities can be a powerful tool for students to explore professional clinical complexity and uncertainty when taught in a transdisciplinary way. In this session, uncertainty operated on several different levels: the introduction of unfamiliar concepts, materials, and methods to students, transdisciplinary approaches to teaching, and the complexities of real-life clinical practice. Further, we argue that to manage uncertainty, medical students must cross from a scientific training based on positivist understandings of evidence and knowledge, to one which foregrounds multiplicity, nuance, interpretive critical thinking, and which understands knowledge as contingent and contextually produced. In facilitating such learning, it is crucial that the teaching team includes experts from both medical and humanities fields to scaffold student learning in an intellectually dynamic way, drawing on their disciplinary knowledge and wide range of personal professional experiences.
- graphic medicine
- medical education
- medical humanities
- narrative medicine
Data availability statement
No data are available. Participants did not consent to data sharing.
Statistics from Altmetric.com
Medical humanities in medical education
What are the skills required by the 21st-century clinician to deliver the best person-centred care? Moreover, to what extent is it essential to recover a model of medicine that sees it as an ‘art’ as well as a ‘science’ (Wald, McFarland, and Markovina 2018)? Can biomedical training alone deliver competent and compassionate doctors? These questions bring us to the difficult, contested terrain that we might describe as the borderlands between medicine and the humanities disciplines.
Medical humanities and medical education continue to have a complicated, and sometimes fraught, relationship. One of the key recent drives within the field of medical humanities, towards a model of ‘critical medical humanities’, has taken issue with what Viney, Callard, and Woods (2015) describe as the ‘service or utilitarian mode’ in which the humanities is deemed by medicine to have an additive or restorative effect. In this model, the humanities is called on to ‘(humanise) the objectivity of biomedicine’ (Viney, Callard, and Woods 2015, 3) and ‘play a role’, rather than participate as an equal educational partner in the sphere of medical education. Critical medical humanities takes the principle of ‘entanglement’ as one of its core concepts (Fitzgerald and Callard 2016) and eschews the functional engagement of the humanities by medical education. Moving beyond the ‘first wave’ medical humanities approach, which has traditionally focused on ‘effectiveness, in terms of empathy’ and has taken a ‘specific interest in, and concern about, issues of communication’ (Whitehead and Woods 2016, 4), the critical medical humanities would propose a more complex understanding in which these seemingly discreet fields might actually be co-constituted.
From the perspective of the medical education field, it is commonly assumed that the humanities are solely arts-based, and therefore their use in undergraduate medical curricula can be interpreted as ‘edutainment’ (Bleakley 2015, 47). By contrast, Spicer, Harrison, and Winning (2013) argue that all ‘art, critical theory, history, law, literature, music, philosophy, and theology fall under the mantle of medical humanities’ (4) and offer a rather more complex application of social and cultural theories within the curricula of medical education. Current discussions in medical education identify the crucial role of diverse and pluralistic teaching, and from individual sessions to full-scale programmes, the medical humanities are increasingly being built into undergraduate medical curricula. These interventions not only allow students to develop a critical toolkit to deal with the uncertainty, ambiguity and scope for errors that are central to clinical practice, but also offer different lenses with which to explore the skills of reflective practice that are essential for patient care and personal well-being in a medical career (Mangione et al 2018).
Following recommendations by the General Medical Council in 1993 (Spicer, Harrison, and Winning 2013), the practical and conceptual challenges of incorporating the medical humanities into medical school curricula have been explored by several scholars (Macnaughton 2000; Meakin 2005; Shapiro et al 2009). Perhaps the most radical and persuasive rationale for this incorporation, and one which we seek to advance in this article, is the recognition that the epistemological frameworks and practices of the humanities disciplines, alongside those of the biomedical sciences, are in fact essential if medical students are to learn to ‘think like a doctor’ (Chiavaroli 2017, 20). In this recalibration of the relationship between the humanities and medicine, in which the division between them dissolves at the point of real-life clinical practice, we argue that the skill set and epistemological frameworks of the humanities are precisely the tools required to sit alongside a clinical skill set in the practice of medicine.
Notwithstanding the rich potential of drawing on these epistemological frameworks, one of the first and most substantial hurdles faced in medical humanities teaching is the radically different nature of the trainings undertaken in medicine and humanities disciplines. Learning within the humanities disciplines requires medical students to cross from a scientific training based on positivist understandings of evidence and knowledge, to one which foregrounds multiplicity, nuance, interpretative critical thinking, and also understands knowledge as contingent and contextually produced. The desired endpoint of this crossing is the enrichment of students’ capacity to draw on both positivist and critical paradigms, as needed, when it comes to the uncertain, complex world of real-life clinical practice. However, this transitional journey is arduous for students and needs to be carefully scaffolded, with the relevance to clinical practice continually signalled, while humanities disciplinary thinking is taught authentically and without reductive simplification. We strongly endorse the view of Richard Meakin (2005) that ‘educators from both the humanities and medicine need to make the effort to understand each others’ cultures’ (50). It is our contention, as we show in the course of this article, that such teaching is best undertaken dialectically by a teaching team composed of humanities scholars and experienced clinicians who create and teach medical humanities sessions collaboratively.
This article arises from a collaboration between Imperial College London and Birkbeck, University of London, in which medical humanities was embedded into the Imperial College undergraduate medical curriculum. Imperial College London (2020) incorporates earlier clinical placements, providing the opportunity for students to develop personally and professionally through patient interactions in hospital and community settings from the first year. Birkbeck has, for over a decade, pioneered applied medical humanities, in which the humanities disciplines are brought into dialogue with real-life clinical practice. Through the Imperial/Birkbeck collaboration, 24 fifth-year medical students who had enrolled on a pilot longitudinal placement in primary care were introduced to medical humanities through eight 3-hour workshops involving large group discussions and small group activities. These focused on narrative medicine; clinical listening through the lens of sound studies; the languages of health and healing; cultural relativism and health beliefs; medical photography; professionalism, fallibility and clinical uncertainty; and health coaching.
These humanities sessions were codesigned and codelivered by a three-person teaching team drawn from the disciplines of history, literary studies and medicine. With time and space to think laterally, encounter concepts and paradigms from cultural and critical theory, and reflect creatively within a congested curriculum, it was anticipated that students would gain an understanding of how these skills could help them as future doctors. Students could thereby develop a creative and philosophically enquiring practice to enable them to deal with complex clinical presentations and communicate more effectively with patients within broader cultural and social contexts.
Developing these new skills, however, involves challenges. The introduction of unfamiliar humanities lenses can be understandably disconcerting for both clinical tutors and students (Meyer and Land 2003). Due to the subjectivity foregrounded in the humanities, which understands the role of personal beliefs, cultural values and inherent biases in the formation of knowledge, medical students may not immediately identify with non-scientific material and may feel alienated. Students often do not appreciate the limitations of modern medicine, which become more apparent with clinical experience, and can therefore overlook the grey nuances of real-life clinical practice. Hence, students may find it difficult to grasp the uncertainty that is central to medicine and the necessity for space in the curriculum to analyse and develop ways to deal with this challenge. This sense of unease in the face of disciplinary difference is often shared by humanities scholars within medical education. Meakin (2005) has described how taking part in medical humanities teaching may lead to scholars feeling distanced from their main research areas and disciplines. Such scholars also face the additional challenge of adapting their materials for medical education in a way that fully engages students.
In this article, we focus on one of our humanities workshops, on the theme of uncertainty, during which all the authors were present. The workshop used extracts from three graphic novels, which students discussed in small groups of two or three, reporting back on their discussions to the whole class. By drawing on the session transcript and our own reflections on planning and delivering the workshop, this article demonstrates the depth of student engagement and learning that is possible to achieve when humanities is taught authentically and properly integrated into the medical curriculum.
Teaching uncertainty
Arguably, one of the most substantial contributions medical humanities teaching can make to clinical curricula is a more textured understanding of the nature of uncertainty, together with a conceptual framework with which to explore it. One of the humanities disciplines most familiar with uncertainty is literary studies, which has developed many frameworks to theorise the plural and often undecidable meanings of the objects it analyses. Literature, whether in novel, poetic or dramatic form, is perhaps best defined by its openness to multiple interpretations. John Keats, the 19th-century physician and Romantic poet, considers the unique challenges and potentialities of literature, both its writerly creation and its readerly reception, in the following quotation:
several things dovetailed in my mind, & at once it struck me, what quality went to form a Man of Achievement especially in Literature & which Shakespeare possessed so enormously – I mean Negative Capability, that is when a man is capable of being in uncertainties, Mysteries, doubts, without any irritable reaching after fact & reason… (Keats (1958, 193–94))
Keats’ concept of ‘negative capability’, which is not in fact a negative entity but a measure of great ability to bear uncertainty, offers a powerful model for thinking about the kinds of uncertainty that are central to both the learning and the practise of medicine. While certainty might be both a structuring concept and a much-desired aim in medicine, both for clinicians and for patients, the contradictory complexity of medicine in practice is captured by the oncologist Siddhartha Mukherjee (2015) in his observation that the ‘laws of medicine’ are actually ‘uncertainty, imprecision and incompleteness’ (7).
Late 20th-century explorations of the ‘uncertainty’ embedded in language itself, and the complex process by which meaning and sense are made of literary texts, are epitomised by the post-structuralist theorist Roland Barthes. He argues, in his seminal essay ‘The Death of the Author’ (Barthes 1977), that a text is not made by its author but rather its reader, whose individual interpretation of it will be affected by that reader’s experience, identity and subjectivity; one reader’s understanding of the meaning of a text may differ radically from that of another. This is the challenge and the pleasure of literature. For a student of literature, learning to sit with the uncertainty of meaning, its plurality and its contradictions, is a primary critical skill.
Following on from these insights drawn from Keats and Barthes, we contend that the theories of narrative encountered within certain branches of literary theory have much to contribute to teaching about uncertainty in a medical education context. The narratologist Tzvetan Todorov (1969)'s model of narrative structure proposes that any and every narrative will follow a five-part course. In this model, narrative develops from a place of balance (‘equilibrium’), through events that destabilise that balance (‘disequilibrium’), before this destabilisation is acknowledged and resolved, thus re-establishing equilibrium. Intrinsic to this model of narrative is the structuring component of uncertainty. A number of writers have highlighted uncertainty as a central feature of illness and diagnosis. For Ann Oakley (2007), in her book Fracture (2007), a fracture of her right arm becomes the starting point for an exploration of the body in western culture. On her way home after her surgery, she notes: ‘Something has happened to me, but I’m not sure what. … I’m nursing a smashed-up arm and beginning to wonder what impact my ‘impact fracture’ will have on me and my life’ (10). In Illness (2019), Havi Carel (2019) describes her experience of being diagnosed with the rare lung disease, lymphangioleiomyomatosis (LAM). The disruption of equilibrium in Carel’s account is jarring: ‘In the morning, I was still happily navigating the world as a healthy person, although I got breathless easily. That afternoon, I learnt I had LAM’ (77). Her diagnosis necessitates an ‘overhaul (of) all my plans, expectations, goals, projects, and horizons’ (77). In both Oakley’s and Carel’s accounts, narratives of health are disrupted, and ways of being in, and interacting with, the world are renegotiated.
Within medical humanities, discussions and uses of narrative remain contentious. On the one hand, the movement of narrative medicine draws on the understanding that in making sense of our lived experience, and the stories we tell about ourselves to others and about others, narrative is fundamental to human experience. Clinician Rita Charon (2001) argues that ‘narrative competence’, which she describes as ‘the ability to acknowledge, absorb, interpret, and act on the stories and plights of others’ (1897), is essential within clinical practice. By contrast, arguing that ‘the attachment to and valorisation of narrativity is not universally shared’, Angela Woods draws on the philosopher Galen Strawson’s pronouncements ‘against narrativity’ to problematise the narrative turn within medical humanities (Woods 2011, 76). Strawson’s contention that there are ‘deeply non-narrative people’ (Strawson 2004, 429) would seem to require an exploration of ‘non-narrative ways of understanding and articulating the experience of illness and its impact on the self’ (Woods 2011, 76). Beyond these polarised positions, we argue here that more applied encounters with narrative have considerable potential to teach medical students about the nature of clinical uncertainty. We propose that, taking a conceptual step back, students and clinicians first need to understand how deeply complex ‘narrative’ can be – for example, how a patient’s story unfolds in the course of a clinical consultation.
Graphic medicine, which has seen an exponential rise as a popular narrative form in the early 21st century, constitutes a useful tool in the context of exploring narrative uncertainty. Coined by doctor, writer and artist Ian Williams (2007), the term ‘graphic medicine’ refers to the use of comics, graphic novels, and other visual narratives in patient care and medical education. Examples include Brian Fies’ serialised digital work Mom’s Cancer (Fies 2008) and David B.’s graphic novel Epileptic (David 2006). Graphic medicine, in which narratives about illness and medicine are explored from the perspectives of both patients and doctors, connects directly to clinical practice and is accessible to students within a medical education setting. Graphic medical narratives offer representations of lived experience in different ways to patient cases, or clinical narratives, in that they allow students to identify with the different positions of patient, clinician or even family member in a clinical scenario, as characters, rather than as real people. Since our narrative exercise required students to make decisions about reformulating these narratives, as we describe below, the use of published graphic novels removed some of the anxiety of ethical or professional responsibility towards real individuals.
The narratives of graphic medicine are presented through visual, textual and spatial means, with much space left for individual interpretation and reflection on personal experience. The interplay between the panels in a sequence, the literal frames and gutters, often require considerable readerly input in the creation of meaning.1 Careful observational skills and being able to decipher incomplete visual information is akin to clinical reasoning skills involved in the diagnostic process in medicine (Green and Myers 2010). To extend this experience of readerly interpretation, we undertook an exercise with our medical students to make sense of a narrative sequence without context or explanation. Students worked in small groups with an excerpt from David B.’s (2006) Epileptic, Brian Fies’ (2008) Mom’s Cancer, or Sarah Leavitt’s Tangles: A Story about Alzheimer’s, My Mother and Me (Leavitt 2011). First, they read and discussed the extract, and tried to make sense of it. They were then tasked with literally deconstructing the narrative by cutting up single panels or sets of panels with scissors. The group then made collective decisions about how to re-sequence these panels in such a way as to foreground different dimensions of the narrative. In working with an excerpt from Mom’s Cancer (figure 1), for example, one group sought to emphasise the volume of confusing medical information that the patient was faced with by placing several such panels next to one another in a sequence. In another group, an excerpt from Tangles was reworked to remove what the group described as “small talk”, in order to better highlight the key questions that the family of an Alzheimer’s patient may have. This applied and embodied encounter with narrative meaning, the working through of uncertainty and ambiguity, as well as the responsibility to produce authentic narrative accounts of patient and family experience, allowed students to reflect on the nature of the structures, details and contradictions that are fundamental to all human storytelling, including that which takes place in clinical consultations.

Fies (2008), Mom’s Cancer (New York: Abrams ComicArts, 2008), p10 (permission was granted for image use).
In the following sections, we draw on direct quotations from the workshop transcript to explore how uncertainty operated on several different levels during the teaching session. The introduction to students of unfamiliar concepts and materials, coupled with a novel transdisciplinary approach to teaching, allowed for the modelling, exploration, and collective resolution of uncertainty within the session itself. At the same time, the extracts that we selected from the graphic novels encouraged students to consider the multiple subjective narratives, and narrative complexities, that they were likely to encounter in real-life clinical practice.
‘What’s going on?!’: learning through narrative uncertainty
Student 4: So, what was… What’s the whole thing about?
Student 3: [laughs] What’s going on?!
As this student exchange during the narrative exercise suggests, the activity manifested uncertainty in different ways. Uncertainty stemmed from the decontextualised narrative extract with which students were presented, but also from the unusual task they had been given and their own doubts about their ability to complete it. This foregrounding of uncertainty was intentional on our part: using the extracts from the graphic novels provided a non-threatening way into a conversation about uncertainty, without addressing the issue of professional uncertainty immediately (this was discussed later, in the second half of the session). In introducing the exercise, we made students aware that the graphic novel extracts would be difficult to interpret, detached as they were from their original context:
Tutor 2: I’m not going to tell you too much about these stories because I want you to be jettisoned in, as you so often are, with a patient’s history. Presented with something you don’t know. Often, as Colleen Farrell says, you end up in the middle of a narrative. Something’s already… Something’s happening in their life and you’ve got to try and catch up.
In designing the exercise, it was important to us that students were able to discuss and reconfigure the extracts within groups. Socio-cultural theories of learning, such as those proposed by Lev Vygotsky (1978), Etienne Wenger (1991), Jean Lave and Wenger (2002) and Roger Säljö (1999) see learning as a fundamentally social activity. These theories emphasise the importance of dialogue, both between people and internally. By using small-group face-to-face teaching, we were able to maximise ‘the potential for individual or shared reflection’ (Spicer, Harrison, and Winning 2013, 21), as students worked together to negotiate the meanings of the sources before them. The conversation below, from a group working with extracts from Mom’s Cancer, is one of several examples where students could be seen collectively working out their uncertainties about the narrative:
Student 5: Who actually has the cancer?
Student 1 & 2: The mum!
Student 5: No, but isn’t the woman…?
Student 1: No, but…
Student 5: No, but does it actually say that anywhere?
Student 2: Yes, because she’s the bewildered one, so I assume she’s the one with the diagnosis.
Student 5: Oh, okay, I wasn’t sure if it was the child and the mum was just trying to catch up.
As well as a practical step towards developing Keats’ negative capability, the exercise allowed students to put forward various explanations about what was taking place in the narratives and, in doing so, recognise how subjectivity can shape individual interpretation, as in student 2’s statement that ‘We all just had different interpretations here basically!’. These ‘different interpretations’ evolved throughout the session, as students were able to reflect on the extracts while listening to other members of their group and discussions taking place elsewhere within the room. Student 4’s realisation partway through the exercise – ‘Maybe I’ve started picking up on things’ – illustrates the value of giving students the time and space to reflect on narratives and work things out for themselves. Although such interpretive work is a common way of working for humanities scholars, medical students have fewer opportunities to develop the kinds of critical thinking skills that help to illuminate the nuanced and contingent nature of knowledge.
At the end of the exercise, each group was invited to share and explain their reordered narrative. In doing so, the usefulness of shared reflection in groups was clear, as well as the way in which the students’ understandings of the narratives had shifted and developed during the course of the exercise. Discussing their work with Mom’s Cancer, one group explained their thought process and collaboration to tutor 3:
Tutor 3: Tell us why you did it that way, if you can.
Student 2: So, we thought it was quite interesting. In lots of stories, sometimes, they put the ending first. You see how the story ends and then you see the build-up to it.
Student 1: So, we started with that. So, it was your [Student 2’s] idea to do that.
Student 2: Yes, we started with that and then it just kind of flowed from there. We didn’t actually end up like that in the end. So, what it was, we wanted to show the mum’s completely bewildered at first. And then, even more information is being thrown at her. And we thought that we wanted it to try and become more optimistic because the original story was quite pessimistic.
Our own recognition that the narratives might pose an interpretive challenge was important in making students comfortable in volunteering their feelings of uncertainty, both about the narratives and the task itself. There was another level of uncertainty, however, that was present within the session, which is explored in the next section: uncertainty from the perspective of the tutors.
‘You may or may not agree with that’: modelling uncertainty through transdisciplinary teaching
We would argue that the particular teaching model used in this session, and indeed in all the sessions designed in the Imperial/Birkbeck collaboration, illustrates a profound engagement with uncertainty through the dynamic and fluid nature of transdisciplinary coworking. Drawing on our own uncertainties, and the challenges we had faced in our respective fields, was particularly productive as our sessions brought together three experienced teachers from three different disciplinary backgrounds. In running these sessions, none of us alone could have adequately responded to the wide range of issues discussed and questions raised by the students. For example, while one of us was able to offer insights into the diagnosis of a particular condition, another was able to speak about how diagnostic criteria have evolved over time, and another was able to draw on patient experiences through literary examples. As well as clarifying specific points for students, the presence of teachers from different fields was a working illustration of how specialist knowledge may be shared across disciplinary boundaries, constructing new meanings during the process. Such a process, though, also generates a degree of uncertainty, particularly around how the teaching may unfold in the course of a particular discussion. This uncertainty must be held within the teaching team, both with each other and for the student group.
Within our sessions, students were often able to see this continuous process of understanding and negotiating uncertainty in operation as we responded to one another’s ideas, or added further detail to a point. For example, the session began with a discussion of the concept of the ‘unreliable narrator’, a critical term drawn from literary studies, which was then picked up and reconceptualised through the other frames of historical analysis and clinical practice. The following exchange records the circulation of the term through different lenses, and the eventual co-construction between tutors, and indeed also students, about its relevance in the clinical setting:
Tutor 3: So, [Elaine Scarry] is using this kind of literary term [the unreliable narrator] to think about how a patient sits in a clinical encounter. You may or may not agree with that, I think it’s quite a contentious reading of it.
Tutor 1: It’s interesting, Tutor 3, just to add to that.
Tutor 3: Yeah, go on…
Tutor 1: I have seen in case records from the early 20th century, the term about … not ‘narrator’, they don't use [that], but they talk about the patient being a “historian”, in terms of giving their own history.
Student 1: [overlap] Hmmm. Yeah we use that quite a lot.
Student 3: Mmmm
Tutor 1: And it was saying in the notes, often explicitly… have you [speaking to Tutor 2] seen this as well? “The patient is not a reliable historian”…
Student 4: [overlap] Yes, unreliable… or not a very good historian.
Tutor 2: We still write it, don't we?
Student 4: [overlap] Yeah we still do.
This transdisciplinary approach to meaning-making, and negotiation of terms in relation to disciplinary training and experience, foregrounds the principle that uncertainty and plurality are best managed by a collective engaged in ‘dialogue’. In relation to the importance of dialogue in students’ learning processes, Mercer and Howe (2012) expand on the foundational pedagogical theories of Vygotsky (1978), who emphasises the importance of language and dialogue in the learning process. Mercer and Howe (2012) observe that knowledge must be understood as being socially situated and derived, not simply an individual possession but the creation and shared property of a community. We would argue that medical humanities taught through this transdisciplinary model actualises a more democratic construction and acquisition of knowledge, as well as demonstrating the productive management of uncertainty.
Further, we would argue that the transdisciplinary model, and the engagement of students in an embodied and applied engagement with uncertainty, generates new and constructive dynamics of collaborative learning. Educational research shows that different types of conversations, particularly between teachers and students, have different impacts on learning. For example, in their exploration of ‘the science classroom’ in secondary school settings, Scott and Mortimer (2005) distinguish between ‘authoritative’ and ‘dialogical’ interactions. In the former interaction, the ‘authoritative introduction of new ideas’ is used to establish the ‘canonical scientific view’ (605). By contrast, the dialogical interaction allows students to undertake the ‘application and exploration of those ideas’ (Scott and Mortimer 2005, 605). The open exploration of uncertainty within the teaching team, and between the team and students, recalibrates the notion of authoritative interaction, moving away from a positivist model of factual knowledge to the more complex terrain of subjective emotions, in which the affective experience of uncertainty is located.
As the following exchange about Epileptic (figure 2) demonstrates, a ‘levelling out’ between tutors and students occurs. This is evidenced in the sharing of laughter, as uncertainty is identified as a normal and vital part of the narrative exercise, as well as being pervasive, both in clinical practice and other disciplines, and indeed a basic human condition:
Student 4: I thought I knew what I was reading until the first page… Second page and then, and then it just got…
Student 3: What?!?
Student 4: I just don't understand what’s going on!
Student 3: What the hell is going on?
[group laughter]
Tutor 2: Are you confused?
Student 3: Where did Genghis Khan come from?
[group laughter]
Student 4: I guess I…
Tutor 3: [laughs] I know that feeling.
Student 3: Yeah
Tutor 3: The feeling of uncertainty.
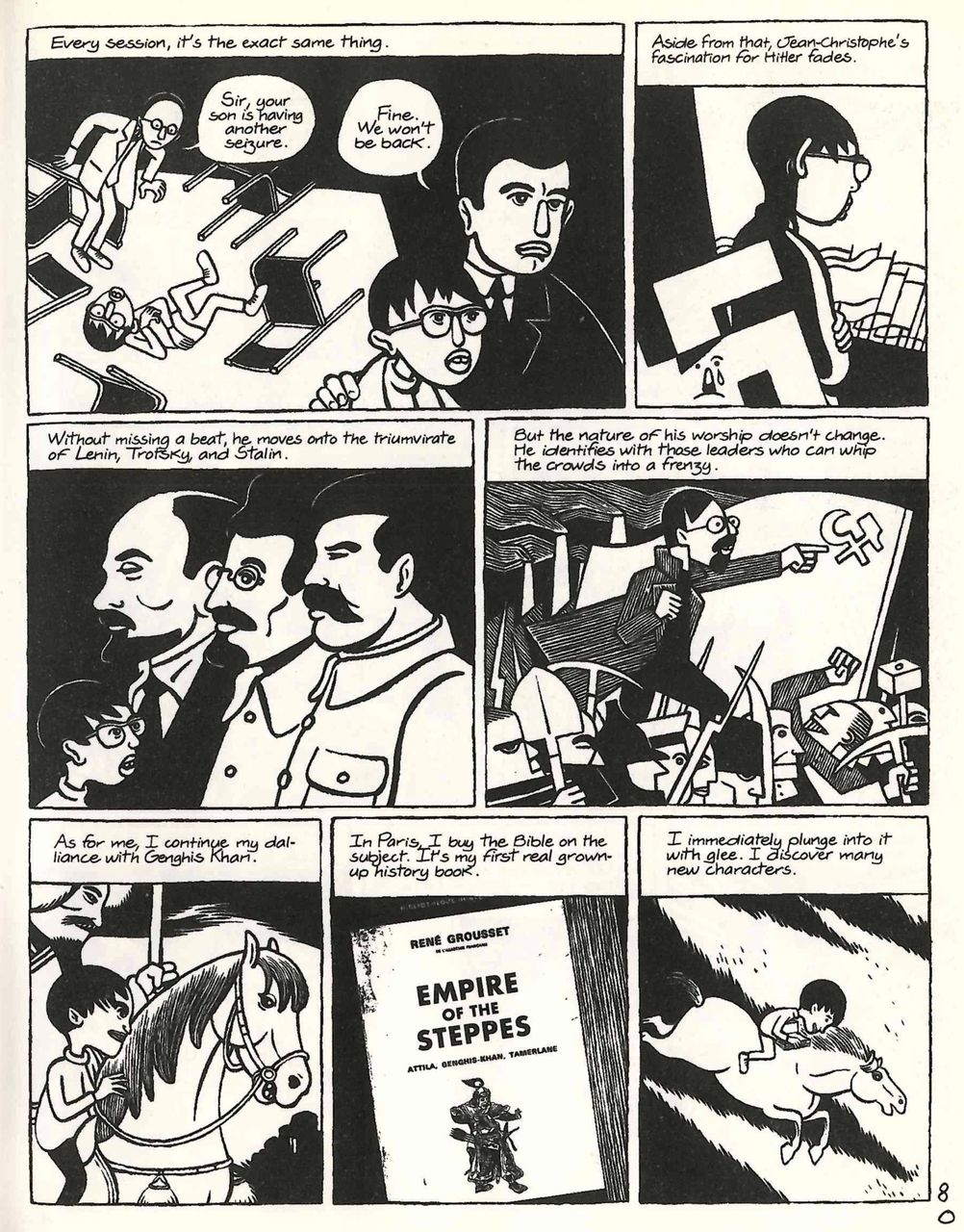
David (2006), Epileptic, trans. Kim Thompson (London: Jonathan Cape, 2006), p80 (permission was granted for image use).
Moreover, we would argue that collaborative learning about uncertainty, using humanities’ materials and skill sets, has a profoundly productive bearing on professional identity formation in the medical context. Molloy and Bearman (2019) assert that medical educators ‘have a role to play in modelling how health professionals negotiate the balance between making themselves vulnerable and maintaining credibility’ (32). Within our sessions, our use of personal anecdotes about uncertainty in our own early and continuing careers allowed students to see that their teachers had struggled with many of the same concepts that they were exploring in the tasks that were before them. All three tutors were forthcoming with anecdotes that related to their professional experience. For example, when students were struggling with the task, tutor 3 recalled that she ‘remember[ed] reading this Virginia Woolf novel as an undergraduate, thinking, I can’t… There’s no story here because it’s all inside people’s heads’. Tutor 2 recalled times of uncertainty with patients as a medical professional. In the following exchange, she describes the uncertainty about how much to allow a patient story to unfold in a consultation bounded by time constraints while also trying not to miss important clinical information2:
Tutor 2: I think more and more with chronic illness, [an] ageing population, you've got patients that live alone and I think getting ill alone is really scary. On the converse, you know I had a similar patient who used to always have tea and biscuits ready for my home visit.
[laughter]
Tutor 2: And it was like: ‘Oh I'm starting a clinic in ten minutes. Just came around to listen to your chest quickly’.
[Student 2: laughs]
[….]
Tutor 2: But they have great narratives! I have one particular patient who is obsessed with swans.2
Student 2: Ahhh
Tutor 2: So we always talk about swans, … but then through that I found out her whole life story about how her husband died in hospital at the age of 40 and how that’s really informed her choice about how she wants to die essentially.
Student 3 & 5: Hmmm
Tutor 2: And it really was quite powerful.
Such stories from personal professional experience, and its endemic uncertainties, offer the recognition that professional identity is an entity in constant flux and reformation. We argue that in undertaking the ‘risk’ of exposing our own thought processes and uncertainties as teachers and as established professionals in our respective fields, we simultaneously recognise the liminal state of professional identity that many medical students see themselves occupying: not quite doctors, but—by virtue of their roles working within clinical settings—not simply students either.
‘She’s got a big tumour sitting in her brain… that’s the reason why she’s not understanding things’: making clinical connections
One of the goals of humanities teaching in medical education is to provide an environment in which students can develop their reflective skills and make connections with their own clinical practice. This process relies on a sense of community being built within the group and the provision of a safe space for students to challenge and exchange personal (and often private) insights and experiences. It is also necessary that we, as tutors, are authentically involved participants within this reflective community rather than simply aloof observers. In our sessions, it was evident that students valued the time to not only reflect on complicated patient encounters but also to explore how varied attitudes and practices in primary and secondary care can affect a patient’s illness journey. One student, for example, remarked that she had ‘a different perspective being a medical student now’.
In appreciation of the challenge of adopting completely new concepts and perspectives, it was imperative that we maintained student engagement during our medical humanities teaching sessions. Clinical relevance was vital not only to make the graphic medicine exercise more accessible for medical students but also to retain their motivation to complete the difficult task. As the session progressed, students became increasingly comfortable with volunteering ideas and anecdotes that explored their personal experiences of uncertainty beyond the group activity, by relating the graphic exercise back to their own patient interactions during clinical placements.
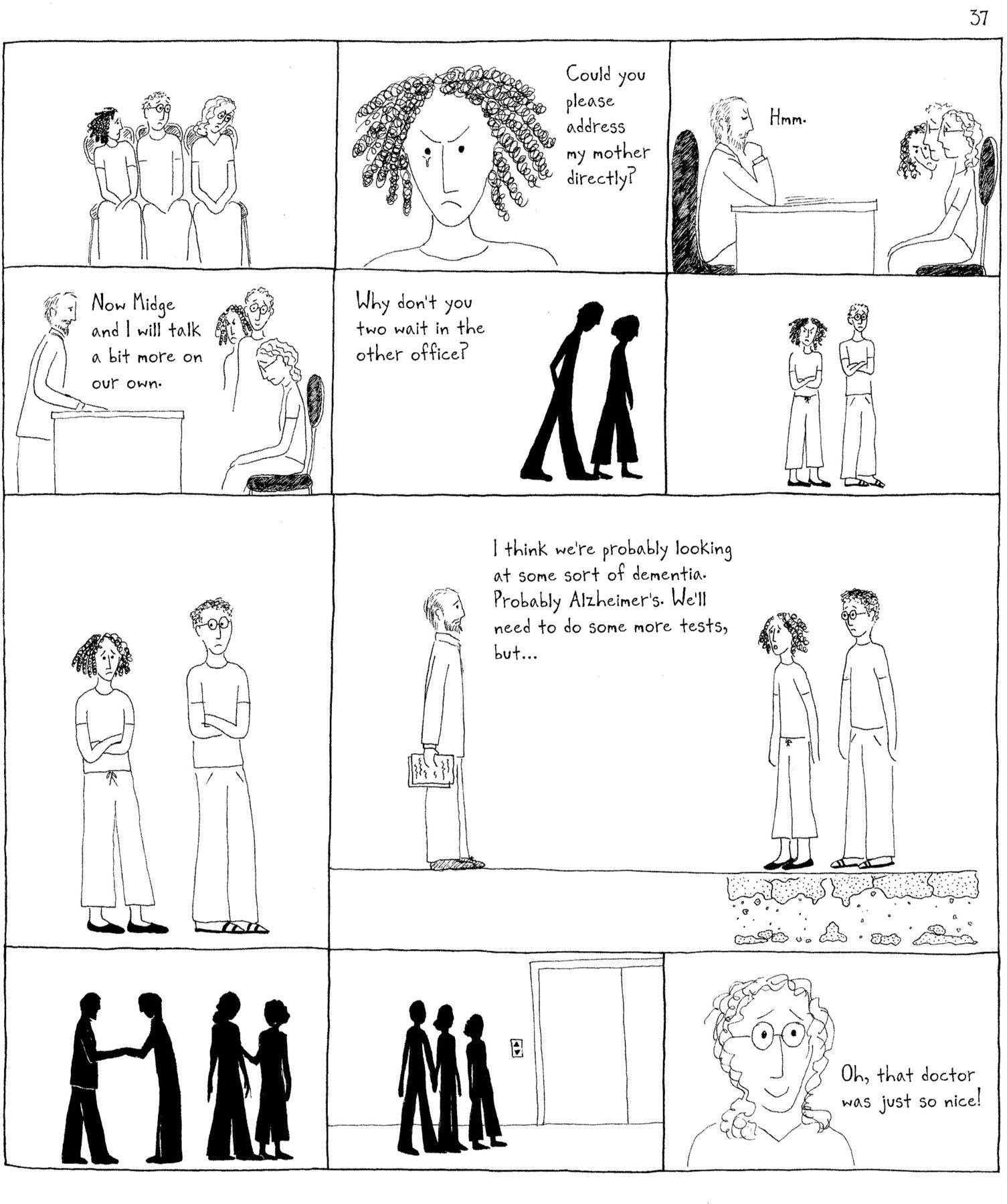
For example, without prompting, through their engagement with Tangles (figure 3), students were quickly able to realise the conflict of agendas between doctor and patient that can occur in clinical consultations, as well as the impact and uncertainty of a lifelong diagnosis from a patient’s perspective:
Student 3: So, we, as medics, we’re always focused on lots of questions we ask, aren't we? There’s lots of small talk, obviously, it’s a big diagnosis you're coming to. But when it boils down to it, if you cut away all the small talk, you’re left with these questions. And the answers to these questions are really what matter… And it’s interesting, it was like, all the different answers, look at the patient [in the exercise], look at her son-in-law, …the whole family unit. And then, all the while, you get to the end of it [the diagnosis], the patient’s still completely oblivious.
{kind=link}
{kind=link}
{kind=link}
Leavitt (2011), Tangles: a Story about Alzheimer’s, My Mother and Me (London: Jonathan Cape, 2011), p37 (permission was granted for image use).
Furthermore, students also examined the communication skills and dynamics within the clinical encounter. This was clearly demonstrated when the students continued to examine the panels in Tangles where the clinician and patient’s family are discussing the patient’s condition while the patient herself remains unaware of it (figure 3). Through the opportunity to view the consultation from a different vantage point, students were able to emotionally engage and identify with the patient’s position. One of the most powerful moments of the teaching session was understanding the students’ irritation that the patient was not being adequately acknowledged. As one exasperated student commented:
And she’s unwell… There’s actually something going on here… It could actually be the fact that she’s got a big tumour sitting in her brain, that’s the reason why she’s not understanding things.
This illustrated that the humanities teaching session offered students an alternative educational space in which they felt comfortable enough to publicly critique the medical profession through the graphic medicine exercise. This unearthing is something that is often kept within the students’ hidden curriculum (Hafferty and Franks 1994).
Drawing on the dialogical learning theory described by Alexander and Wolfe (2008), the secure environment within this teaching session also enabled tutors to facilitate the conversion of unstructured classroom conversation to more purposeful discussion relating back to clinical practice and medical uncertainty. The following dialogue illustrates a discussion between tutors and students connecting the graphic medicine narrative exercise with the messiness and undulating course of real-life clinical practice; uncertainty within medicine can often be a long, arduous journey for both patient and clinician, and consequently, medical students must develop the skills to remain patient themselves and endure the uncertainty during this process:
Tutor 3: Brilliant. So, you really tried to integrate what was quite separate in the narrative and bring it together more – brilliant.
Student 4: Mmm
Student 3: Yes, unintentionally, just…
Tutor 3: It’s almost an unconscious process a lot of the time, isn't it?
Tutor 2: It’s like taking a medical history. We were saying, we repackage it, right? and we present it in a way that we understand it.
Tutor 3: Right… Right
Student 3: Makes sense, yeah
Tutor 2: So, you're still going from A to B, but avoiding the winding roads – basically.
Student 2: Lots of winding roads!
[Tutor 2: laughs]
Tutor 3: Yes, absolutely. Brilliant.
Through negotiating their uncertainty during the graphic medicine exercise, students further developed their reflective skills by contemplating ways in which they could constructively apply lessons learnt during the session to improve their own practice in the future. For example, one of the students spoke of a regular heart-sink patient and powerfully considered the importance of deconstructing his patient’s narrative during forthcoming consultations. He reflected on why his patient often initiated long conversations about subjects completely unrelated to his chronic illness:
I’ve been thinking about it throughout this session. The reason … is because he’s scared, he doesn’t want to talk about medicine. … [I]n a good way, [this session has] helped me to reflect that actually you really do need to listen and understand why people are talking.
This quote was one of many that signified a new realisation for the students that narrative attentiveness from different perspectives, and subsequent personal reflection, can transform a frustrating patient encounter into one with a deeper humanistic connection and understanding. As modern medicine moves from the cure of disease to the management of chronic illness, it is vital that students remain attuned to patient narratives and develop their capacity to tolerate clinical uncertainty, so that they are able to competently navigate complex medical journeys in partnership with their patients.
Conclusion
In this article, we have argued for the medical humanities as a powerful medium through which to enrich medical students’ learning, particularly in relation to concepts and skills that have been identified as core competencies in medical school training (General Medical Council 2018), such as ‘dealing with complexity and uncertainty’ (8). What matters, however, is the mode in which medical humanities is delivered and the status conferred on such teaching. As Jane Macnaughton (2000) has written, there is a danger of medical humanities courses being seen as ‘club[s] for interested people’ (26), unrelated to the business of medical education as a whole or as having anything specific to teach students in preparation for their future careers. Similarly, we faced challenges of sporadic student attendance and a degree of ‘competition’ with revision sessions for clinical exams. The pressure of timetabling means that medical humanities teaching is often unintentionally presented as an add-on to ‘real’ medical teaching. Our experience, like many others within the discipline, is that the limited time available for the medical humanities has a significant impact on perceptions of the discipline’s usefulness. Students are given a session of 1 or 2 hours—in addition to their other teaching and clinical commitments—within which they are encouraged to explore concepts from the humanities that may be entirely alien to them. When students understandably find such concepts difficult to grasp or do not see the humanities as relevant to their own experience, it is all too easy to dismiss medical humanities as unhelpful. Yet, like any other new discipline, students need to be given adequate time and a sustained course of study to familiarise themselves with new concepts, models and approaches (Louis-Courvoisier and Wenger 2005). Moreover, it is crucial that the teaching team includes experts from both medical and humanities fields to scaffold student learning in an intellectually dynamic and authentic way, drawing on their disciplinary knowledge and wide range of personal professional experiences.
Michael J. Green et al (2016) highlight that imaginative and innovative exercises can enable medical students to foster and develop skills in reflection and resilience; ‘creating something new requires medical students to take risks and even to fail – something they are neither accustomed to, nor comfortable with doing … in a way that doesn’t threaten their evolving (and therefore fragile) professional identities’ (483). In this article, through one practical example, we have shown how the skill of managing uncertainty within medicine is extremely effectively taught by drawing on humanities frameworks and sources. The presence of a transdisciplinary teaching team is crucial in exploring these frameworks and sources, allowing for meaningful connections to be made between the humanities and clinical experience, but also creating a space where the state of uncertainty can be openly recognised and explored. During our graphic medicine exercise, students felt completely lost at the outset. However, with the support and collaboration of their peers, and the containment of a transdisciplinary teaching team modelling the management of uncertainty, they were able to make sense of the task, as well as initiate change in their own personal practice. Students underwent a transformation from initial confusion, through enthusiastic engagement, to the application of critical thinking to real-life clinical examples. This represents a journey from ways of knowing foregrounded in the positivism of biomedical science, to the different models of knowledge which foreground multiplicity and nuance within the humanities disciplines. We argue that students need to understand that both sets of knowledge, and the skills embedded within them, are core to attuned and effective clinical practice. This is the fundamental contribution of applied medical humanities teaching.
Data availability statement
No data are available. Participants did not consent to data sharing.
Ethics statements
Patient consent for publication
Ethics approval
Students in the session gave their permission for their verbal contributions to be audio-recorded, transcribed and used in published research. Ethical clearance for this was given by Imperial’s Medical Education Ethics Committee, Faculty Education Office (Medicine), Imperial College London (Application Number: MEEC1819-146).
Acknowledgments
We are very grateful to the students who consented to have their contributions recorded, as well as for their engagement throughout all of our humanities sessions, without which this article could not have happened. We also thank Dr Molly Fyfe (senior academic fellow, Medical Education Research and Innovation Centre (MEdIC), Department of Primary Care and Public Health, Imperial College London) for her helpful reading suggestions and arranging audio-transcription of the session, and Dr Jo Horsburgh (lead for Medical Education Research, MEdIC, Department of Primary Care and Public Health, Imperial College London) for reviewing a draft version of this article. Finally, we also especially acknowledge Dr Sonia Kumar (Director of Undergraduate Primary Care Education and MEdIC, Department of Primary Care and Public Health, Imperial College London) for her initial conception of the Imperial/Birkbeck collaboration, her support of this project and for reading a draft of this article.
Notes
1. In a graphic novel or comic, a ‘panel’ refers to a visual segment, usually placed in a sequence with other panels. A ‘frame’ refers to the lines or borders that outline a panel. A ‘gutter’ refers to the space between framed panels.
2. Subject matter changed to maintain patient confidentiality.
Bibliography
Footnotes
Twitter @NeepaThacker, @harbottlestores, @jolowinning
Contributors All three authors contributed in terms of conducting the research, data analysis and writing this article.
Funding This article presents independent research supported by the National Institute for Health Research under the Applied Health Research programme for North West London.
Competing interests None declared.
Patient and public involvement Patients and/or the public were not involved in the design, conduct, reporting or dissemination plans of this research.
Provenance and peer review Not commissioned; externally peer reviewed.