Article Text

Abstract
Healthcare systems redesign and service improvement approaches are adopting participatory tools, techniques and mindsets. Participatory methods increasingly used in healthcare improvement coalesce around the concept of coproduction, and related practices of cocreation, codesign and coinnovation. These participatory methods have become the new Zeitgeist—the spirit of our times in quality improvement. The rationale for this new spirit of participation relates to voice and engagement (those with lived experience should be engaged in processes of development, redesign and improvements), empowerment (engagement in codesign and coproduction has positive individual and societal benefits) and advancement (quality of life and other health outcomes and experiences of services for everyone involved should improve as a result). This paper introduces Mental Health Experience Co-design (MH ECO), a peer designed and led adapted form of Experience-based Co-design (EBCD) developed in Australia. MH ECO is said to facilitate empowerment, foster trust, develop autonomy, self-determination and choice for people living with mental illnesses and their carers, including staff at mental health services. Little information exists about the underlying mechanisms of change; the entities, processes and structures that underpin MH ECO and similar EBCD studies. To address this, we identified eight possible mechanisms from an assessment of the activities and outcomes of MH ECO and a review of existing published evaluations. The eight mechanisms, recognition, dialogue, cooperation, accountability, mobilisation, enactment, creativity and attainment, are discussed within an ‘explanatory theoretical model of change’ that details these and ideal relational transitions that might be observed or not with MH ECO or other EBCD studies. We critically appraise the sociocultural and political movement in coproduction and draw on interdisciplinary theories from the humanities—narrative theory, dialogical ethics, cooperative and empowerment theory. The model advances theoretical thinking in coproduction beyond motivations and towards identifying underlying processes and entities that might impact on process and outcome.
Trial registration number The Australian and New Zealand Clinical Trials Registry, ACTRN12614000457640 (results).
- medical humanities
- mental health care
- philosophy of medicine/health care
- social science
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
The new Zeitgeist: participation
The current preoccupation with methods for citizen engagement, public participation and involvement of people with lived experience in health system redesign and service improvement might be said to represent the new Zeitgeist—the spirit of our times. 1 Participation has become a distinct cultural and political movement characterised by user involvement in healthcare across a continuum encompassing shared decision-making in clinical treatments and management, quality improvement, service redesign and evaluation. This movement has seen a proliferation of approaches in healthcare quality improvement that use coproduction and related (though distinct) models of codesign, coinnovation and cocreation. The term coproduction historically referred to ‘citizens as coproducers’ of public goods and services, the roots of which can be traced to public administration discourses of the 1970s.1 In this context, citizens were seen to be coproducers of government-funded and delivered public services and by their engagement in service use and delivery, citizens created a public benefit or value.2 In recent times, coproduction has been applied more directly to clients (or service users) of an organisation (both public and privately funded) who engage in coproducing goods and services. The value generated in this exchange might be said to differ and be largely private since most benefits produced from involvement in the production of goods and services are to the client and organisation.2 3 Coproduction has gradually been integrated into public infrastructures procurement and management, and is said to generate better outcomes and optimal utilisation; however, the empirical evidence for demonstrable outcomes is limited.3 4 What is evident is a political and sociocultural mindset shift from ‘experts know and decide everything’ to ‘we need to decide things together’. Authors in the USA have commented that ‘if the healthcare reformation movement has accomplished any significant change indelibly seared to the American culture and Zeitgeist, it’s this: ‘patients’ no longer remain detached spectators in the care they receive.’5 While participation in healthcare is apparent on a number of fronts, it by no means follows that the spirit of participation has become normative and embedded within the design processes and service improvement efforts of healthcare organisations or systems. What is notable though is increased reference to the importance of coproduced services particularly in mental healthcare policies in the UK, Australia, Canada and other Western nations6–9 as well as in low/middle-income countries particularly in response to a lack of government provision of such services.10 11
Involvement in public governance and participation in health systems redesign and service improvement are certainly not solely 21st-century concepts.2 Looking back over the past 30 years there is a discernible ‘period’ of public involvement in service redesign and improvement efforts. In the UK, the establishment of INVOLVE (a national advisory group to support public involvement in health and social care research) heralded a new era for public and patient participation in healthcare research.12 Evidence of the involvement push in service improvement and redesign efforts is apparent in mental health policy from the 1990s and was most recently expressed in the United Nations (UN) special report on the right of everyone to the enjoyment of the highest attainable standard of physical and mental health.6 7 9 13 The UN report referenced the empowerment of people with mental health needs as critical to improving conditions of treatment and support. To achieve this, the report outlined that self-advocacy, peer support networks, trialogues and methods of working such as coproduction were essential to ensure representation and meaningful participation in health service development and provision.8 The pattern repeats in Berwick’s recent call to arms for a third (and moral) era in medicine and healthcare:
…(T)he more patients and families become empowered, shaping their care, the better that care becomes, and the lower the costs. Clinicians, and those who train them, should learn how to ask less, ‘What is the matter with you?’ and more, ‘What matters to you?’ ‘Co-production’, ‘co-design’ and person-centred care are among the new watchwords, and professionals and those who train them, should master those ideas and embrace the transfer of control over people’s lives to the people.14
Three transitions are notable in these developments. First, healthcare recipients are no longer just spectators in their care and, second, their closer involvement is assumed to produce value (how much this is public or private has not been established). Third, coproduction and codesign are emerging as means to facilitate various ends including, but not limited to, both greater individual control and system efficiencies. Clarke et al 15 have cautioned that ‘coproduction’ (and associated variants) may already be in danger of losing meaning as it enters mainstream management discourse and practice. Recent academic critiques of coproduction echo this highlighting a lack of critical engagement with issues of power, power relations and questions of representation in coproduction and codesign approaches. These critiques signal a need to address questions around whether participation fosters inclusion or reinstates existing social exclusions. Or, if the instruments thought to be alternatives to the social structure have become tools that serve the dominant agents.16 Consequently, service user empowerment and democratisation of service provision through coproduction is seen to be at risk of being deployed simplistically.17 18 The ‘dark side’ of coproduction has been noted, where inequities may be reinforced, particularly if they take the form of a substitution of labour and are used solely to provide cover for political decisions.19 Brandsen and Honingh20 have argued that public participation and collaboration on the one hand may be attributed to an emerging public governance paradigm where citizens are engaged in democratic processes and given a voice in governance and decision-making. On the other hand, this involvement could be seen as attempts to harness societal and citizen efforts as a response to dwindling government resources,19 a perceived loss of public value and trust in government services, and a drive to reinvigorate voluntary participation and strengthen social cohesion as a response to fragmentation and a highly individualised society.17 20 Others have argued that, while well intentioned, the implementation of coproduction in the healthcare sector and particularly in mental health remains uncritical:
…the shift towards greater user involvement is typically couched by its advocates as being ethically straightforward and as an unalloyed good, because it represents a transformation of users from a role of passivity and dependence on the paternalism of professionals to more active, empowered and respected autonomous persons …[this] fail[s] to represent the ethical complexities embedded in welfare [and service] relationships.21
Bringing people together to redesign and improve services as coproducers is indeed recreating the ways in which public governance, policy and health services are enacted and function. It is also changing the relationships between providers and recipients of those services. Renedo et al have identified that when involved in improvement, people come to think and act in new spheres of organisational cultures. Quoting work of Cornwall and Gaventa (2000, p 50), they argued, “people make a transition from being ‘users and choosers’ to being ‘makers and shapers’.”22 This transition is not always easy and the social and cultural context must be accounted for. In mental health services, people are no longer seen to be passive recipients of services, they have been reframed as designers, learners and actors who shape the outcomes that they desire from organisations.23 24 In this regard, the participatory Zeitgeist is characterised by an increased focus on coproduction and codesign approaches, and an acknowledgement that people with lived experience must be central in decision-making.25 More than this, experience has become a form of expert knowledge viewed as an essential part of some coproduction processes, particularly those facilitated within mental health or settings where people’s voices have been largely unheard due to dominant institutional and social forces at play. This confluence of approaches and agendas is challenging since coproducers have diverse values, needs and priorities generally,4 and people with lived experience are not a cohesive and homogenous group.26 How the coproduction field grapples with these differences and possible conflicts is important to the healthcare improvement era. Currently though theoretical models that assist to evaluate and explain the engagement, diversity and transitionary experiences of people in coproduction efforts are lacking.
In the mental healthcare setting coproduction and Experience-based Co-design (EBCD) in particular offers a way to shift power dynamics. EBCD follows six stages to identify the positive experiences in services and the areas for improvements (called touch points) and then undertake a codesign process to implement improvements with staff, service users and carers.23 EBCD is qualitative in orientation and has appeal for people who may have experienced health systems as largely paternalistic, dominating forces with a disregard for their views and values; an experience that has unfortunately been all too common for many people living with mental illness and their carers. This disregard of voice and experience has been a major impetus for the growth of the service user/survivor movement which has served also to raise awareness of the importance of lived experience in service redesign and quality improvement efforts. Despite the increase in peer networks and embedded models of service users within quality improvement initiatives as demonstrated by researchnet in the UK,25 Tomes has noted that the ability to redistribute power to ‘end users in a fragmented, politicised health care system remains a daunting prospect.’27 Coupled with this is the risk of essentialising lived experience by use of the term as an umbrella and universal concept.26
It is time to critically evaluate the participatory Zeitgeist as it is being enacted in mental health systems redesign and quality improvement efforts. Greater explication and examination of the claimed outcomes and sustained impacts of coproduction in healthcare is required to advance the field theoretically and practically.1 This includes developing a deeper understanding of people’s experiences of the transition from ‘users and choosers’ to ‘makers and shapers’.22 In the examination of such transitions it must be acknowledged that participation experiences are not universal, organisational cultures are diverse and the direction may not always be from user to maker. To fully examine outcomes and explore processes of coproduction using theoretical models, it is necessary to identify the mechanisms, those ‘underlying entities, processes, or structures which [may] operate in particular contexts to generate outcomes of interest.’28 In coproduction generally there has been less attention to the identification of mechanisms. A survey conducted across the UK, France, Germany, Denmark and the Czech Republic of the coproduction behaviours of citizens with respect to public services related to neighbourhood safety, the environment and health found that intrinsic reward—the belief that citizens can make a difference—was a determinant for coproduction. Results did have contextual variation across nations but largely indicated that where there was an awareness of government shortfalls in performance, coproduction was more likely.29 A repeat of the same survey in Australia also identified that citizens who thought that they could make a bigger difference reported higher levels of coproduction although the factors that contributed to this varied.3 While this highlights some of the motivations for involvement in coproduction of public services, the literature from healthcare improvement projects using EBCD and coproduction remains mostly qualitative and largely comprises thousands of case studies that are strong on the nature and level of coproduction but weak on wider, long-term impacts.30 Studies suggest service outcomes can be transformed without increasing costs, but this has not been systematically evaluated.30 A systematic review of coproduction and cocreation approaches in the public sector drew similar conclusions; process and factors for success have been given a lot of attention but there is less evidence for outcomes.31
Similarly, evaluations of completed EBCD projects in the UK in particular have documented improvements in operational efficiencies, interpersonal dynamics of care, reduced complaints and better communication, team relationships and service users feeling listened to and involved.32 The majority of these studies have been within hospital settings,33 specifically in head and neck cancer services, breast and lung cancer services, gynaecology and colorectal,34 35 lung cancer and intensive care units,34 stroke rehabilitation15 and end of life care in emergency departments.36 A few studies have been conducted in the mental health setting but these are limited.32 33 EBCD evaluations have examined: the processes of EBCD employed, the potential outcomes, the codesigned improvements and their implementation, including sustainability and spread. Despite the documented potential individual level outcomes related to increased self-determination and agency, empowerment, hope, trust, confidence,6 9 improved accessibility and acceptability of services, quality of life13 37 38 and clinical effectiveness and patient safety,39 the evidence to support these outcomes is limited and explorations of the mechanisms which may bring about these outcomes, or assist to explain change or no change are scant.
In health and medical research, the randomised controlled trial (RCT) is upheld as the gold standard for generating such evidence about outcomes. Only one RCT of an EBCD approach has been completed testing if a method called Mental Health Experience Co-design (MH ECO) developed in Australia improves psychosocial recovery outcomes for people experiencing severe mental illness (schizophrenia, bi-polar disorder, psychosis, and major depressive disorder).40–42 In this paper, we use the MH ECO example to build an explanatory theoretical model of change that will assist in the future evaluation of the trial outcomes for MH ECO and provide a basis for further understanding and examination of coproduction and other EBCD studies in the future. In terms of the latter, it is anticipated that this current proposed model is preliminary and would undergo further expansion, reduction and/or refinements as it is applied to other studies in different settings using other EBCD approaches. Before outlining the explanatory theoretical model of change, we provide an overview of the example from which this was developed, MH ECO and its origins.
Mental Health Experience Co-design
MH ECO is an example of a service user and carer peer developed and led systems redesign and quality improvement methodology; it is the first EBCD informed intervention to be tested within an RCT design in the world. The impetus for development of MH ECO began in 2006 partly as a response to the wider sociocultural and political movement to involve and embed people with lived experience in service redesign and quality improvement. The Victorian State government had identified a need for involvement of service users and carers of mental health services in treatment and care planning. There had also been the development of Australian National Standards for Mental Health Services which detailed the importance of service user and carer involvement in service planning, system redesign and evaluation.43 There was also dissatisfaction with standard methods for collecting feedback on public mental health services based on a survey which historically had small response rates and did not adequately capture the experiences of service users and carers; an issue previously noted within quality improvement fields.44
The original tripartite partnership between the peak service user and carer agencies (the Victorian Mental Illness Awareness Council and Tandem representing mental health carers) and State government began, then, with the goal of increasing participation and representation of service users and carers in the annual experiences of public mental health services survey. This involved identification of areas of importance for service users and carers about the kinds of experiences that people thought were important to find out about. The survey underwent testing and piloting for redesignand was administered by telephone. Following its completion, the next step was the development of MH ECO as a quality improvement approach.43 45 The government agency responsible held the view that data alone were not enough—resourcing and action for change would also be required.
The decision was made to pilot the development of a quality improvement methodology using the EBCD model published in the UK in one of the participating non-clinical community mental health support service organisations from the survey redesign project.45 MH ECO drew on the existing EBCD model used within the National Health Service in the UK primarily because the service user or person with lived experience was situated within the design process and it offered guidance on a participatory but structured approach to bring staff, service users and carers together to collaborate for changes.46 The MH ECO methodology development did not begin however with the traditional EBCD information gathering stages of observations or face-to-face, or in-depth narrative interviews and films with service users and carers. Instead, experience findings and the top three touch points identified from the survey were identified for use23 32 34; it is important to note though that the final MH ECO model included the option for in-depth interviews, development of personal stories and for services to adopt different methods for gathering information about experiences. The identification of touch points from pre-existing experiences data was also used within a study completed in the psychiatric inpatient setting where existing in-depth interview transcripts were analysed and touch points developed before codesign work commenced.32 Films were not created for the MH ECO pilot because of limitations of time and feedback from service users who felt that watching themselves on film was uncomfortable.
Table 1 provides an overview of the final format for the MH ECO methodology. It shows the establishment phase, the collection of experiences, the exploration of touch points using a focus group approach, the use of collaboration groups and codesign working groups and a final celebration event. MH ECO also adopts a highly structured approach with peers with lived experience facilitating focus groups, collaboration group and codesign group meetings. Within these meetings participants adopt different roles and responsibilities but the codesign process is always facilitated.
The MH ECO methodology
After the pilot was completed, MH ECO was further adapted for delivery within a cluster RCT to determine its effectiveness for improving psychosocial recovery outcomes for people living with severe mental illness. This was premised on the early pilot findings of increased self-determination, empowerment, hope and positive experiences and how these concepts fit with current conceptions of psychosocial recovery.42 47 As has been shown before, the trial involved a multidisciplinary team of investigators trained in the humanities, applied ethics, primary care, psychiatry, sociology and quality and safety improvement. The original peak agencies responsible for the development of the MH ECO model were engaged as partners (VMIAC an
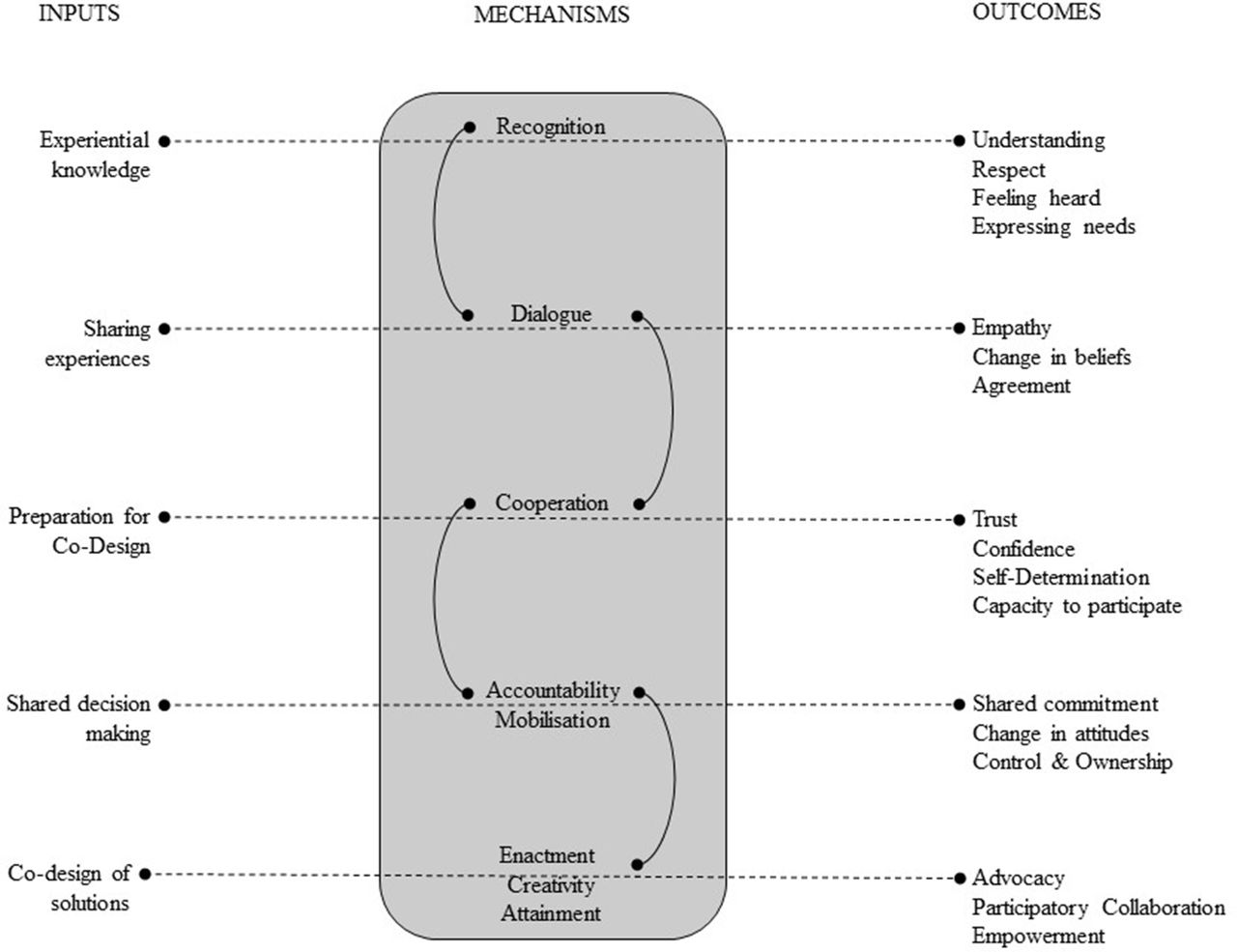
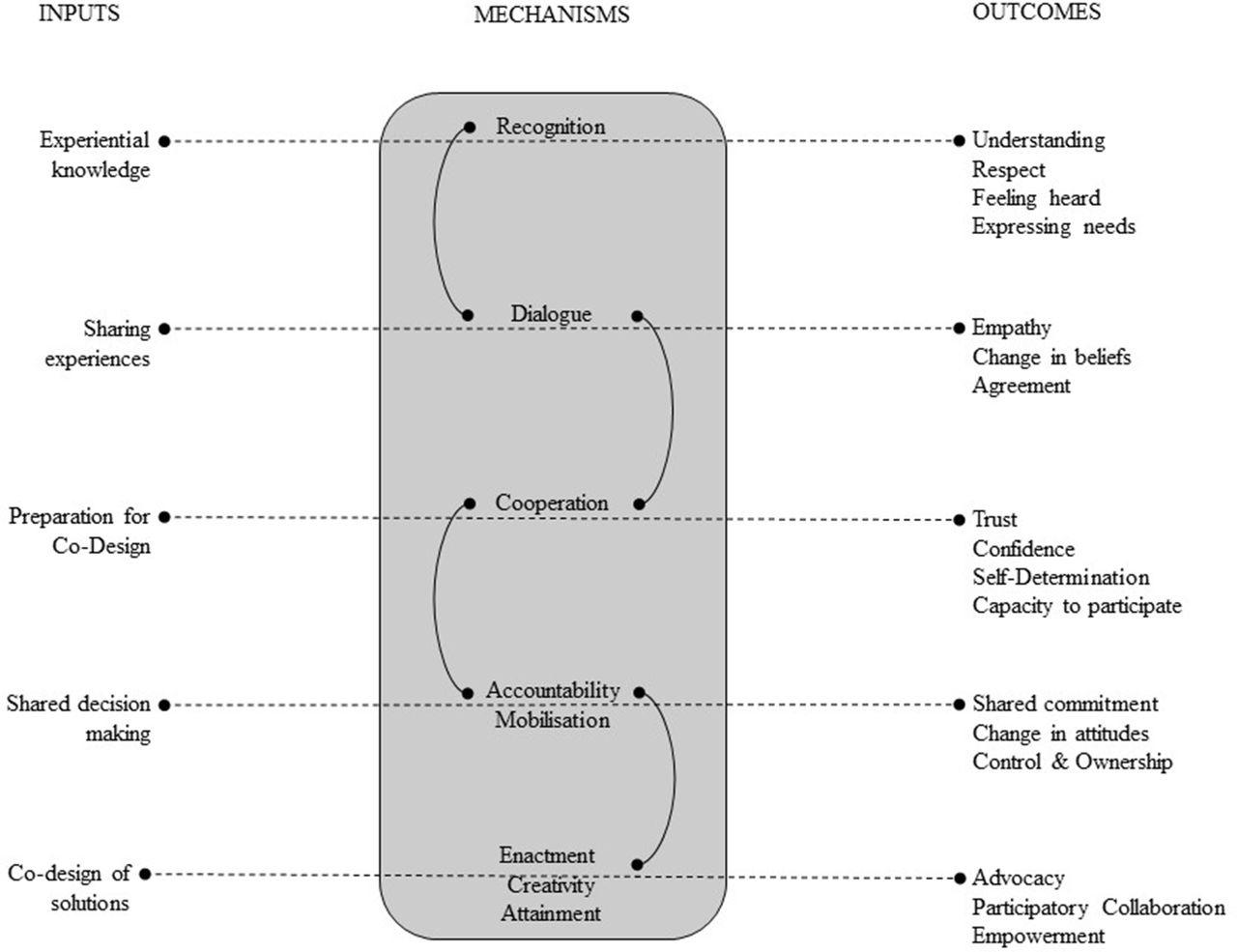
d Tandem)) and two nominated persons with lived experience facilitated the delivery of MH ECO in the trial. Those facilitators and the broader research team were engaged in the process of identifying anticipated outcomes from MH ECO which were presented in a programme logic model developed for the trial. The research team collectively reviewed the inputs of MH ECO (the information gathering and codesign activities, and processes) and considered these against the anticipated outcomes from the programme logic model combined with existing findings in published EBCD evaluations. Eight mechanisms were identified as the potential ‘underlying entities, processes, or structures’ operating within MH ECO. These were discussed by the research team and agreements were reached on how these mechanisms might be essential to generating the anticipated outcomes of MH ECO. The mechanisms were organised in figure 1 as a way to show the flow of mechanisms against stages, activities and process of the methodology. Importantly, the connected lines signify interconnectedness between mechanisms rather than a distinct linear flow where one mechanism might move on to the next.
{kind=link}
The eight mechanisms of change identified within Mental Health Experience Co-design methodology.
It is important to note that the eight mechanisms—recognition, dialogue, cooperation, accountability, mobilisation, enactment, creativity and attainment—do not exist in isolation, there is complexity of the environment and organisational contexts which shape these. In addition, the mechanisms coexist within the relational context of EBCD work. Table 2 presents the mechanisms within an explanatory theoretical model. The explanatory theoretical model shows the inter-relationship between mechanisms and what the research team has identified as a series of ideal relational transitions that could occur in coproduction and codesign activities. Combined, mechanisms and transitions help to explain, examine and understand the processes of codesign (in this case the example of MH ECO is used) and their relationship with outcomes more directly. In future work, in examining the processes and outcomes of activities using codesign the model itself may be refined with new mechanisms identified and relational transitions considered.
An explanatory theoretical model of change for an experience-based codesign approach
Narrative theory and epistemic justice
The explanatory theoretical model begins with an idealised (or perhaps more accurately even a non-ideal) version of an ‘I’ that suggests when service users, carers and staff begin the codesign journey their experiences may be presented as part of narrative of a separated or isolated self. It should be noted that this relational positioning is idealised and in reality people may come to a coproduction or codesign process starting at a different point; not everyone will see themselves in this way. There may be people who are more oriented towards ‘You’ or ‘Us’ in their relationships; the point here is more in the explanatory potential of the relational transitions. Use of the model may assist to highlight the different starting points of individuals, including acknowledging how their own contextual factors and backgrounds might shape this. The explanatory model may then assist to document and evaluate whether the shifts and transitions do occur and, importantly because of the identification of mechanisms coupled with these, whether or not those shifts and transitions were made possible because of different relational capacities.
Our explanatory theoretical model commences with ’I' because codesign projects do start with a focus on ‘I’—service users are asked what happened. What services did you receive? How was your care experienced? What could improve? Equally carers are asked for their stories about their experiences of the system or service. This is an essential step in EBCD studies in contrast to other coproduction activities, as these preliminary stories enable the identification of individual touch points and from this, we can establish those touch points which are shared across people. The beginning point for EBCD is how services or healthcare could be better experienced. Thus, the early stories elicited can naturally hinge on a separated ‘I’ being the main protagonist as people draw on memories of negative experiences; it does not mean that people have not shared a collective story about positive experiences, however the improvement process focuses on what could be better and engages people in a collective response to this. The ‘I’ story can thus be one that is pitted against ‘Them’ but it does not always have to be, there are many variations in how stories are recounted by participants and sometimes people enlist ‘Us’ as pitted against them to foster collective power. It is important to note that there are positive stories within these that are often shared but the focus for improvements is on the negative.
The importance of using ‘I’ and ‘Them’ as a basis for the beginning of the explanatory theoretical model is individuals (I) come together with others to share stories of experience. What’s made possible from this is a sense of collective identity formation. Sharing stories does not make relationships equal or automatically disrupt power imbalances, but stories do enable shared experiences to become part of a collective identity forming process. Narrative theory is thus essential to EBCD and allows the connection between storytelling and identity formation to be acknowledged; this is the case also in the MH ECO methodology. Storytelling offers the opportunity for people to recognise that some experiences are shared by others and people can start to appreciate there are limitations for change, or ways in which broader social and organisational forces constrain the best possible experience of care being in place. Storytelling does not always mean that people automatically feel a sense of shared experience, but listening is facilitated by the recognition of the importance of each other’s experience. For stories to do their work of helping people to move out of a focus on ‘I’ (where it does exist) and a possible viewpoint of their world as pitted against ‘Them’ the mechanism of recognition is essential. When recognition is present it is more likely for the relational transition from ‘I’ and ‘Them’ to occur; ‘You’ may come into focus. This recognition is signalled in the valuing of experience and a recognising effort on the part of individuals to hear the story of experience differently.
This potential relational shift and the role of recognition inherent to it creates what Miranda Fricker calls epistemic justice.48 Fricker distinguished between two forms of epistemic injustice: testimonial injustice and hermeneutic injustice. Testimonial injustices are those injustices that occur when a person’s word is afforded less credibility or their knowledge invalidated through discounting or diminishing their account because of prejudice. Hermeneutic injustice is when the meaning of experience is downgraded and interpreted incorrectly. Examples of this are when collective understandings are skewed by experiences being discredited, or downplayed because of acuity of illness or individuals being framed as not being able to understand the complex procedures within organisations. Recognition that both kinds of injustices have usually been experienced by service users and carers in the mental health setting is critical and similarly staff may have had such experiences; Fricker’s point is that some groups are more likely than others to experience testimonial or hermeneutic injustices. Fricker’s argument is that power asymmetries skew our collective understandings such that the understandings of the more powerful social groups dominate; the task of codesign work is to align symmetries.15 Recognition is thus considered to be a mechanism important to codesign outcomes because it has an enabling function in terms of facilitation of movement between people to an understanding of experience where epistemic justice is present. The mechanism is seen to be one of the critical elements of the explanatory theoretical model because without this shared understanding may not eventuate and without shared understanding there could be limitations in how people work together to enact the codesign of improvements.
Dialogical ethics and narrative contract
The explanatory theoretical model illustrates that in the ideal, groups can create conditions where testimonial and hermeneutic injustices are countered because people to feel heard and valued; people can experience this because the mechanism of recognition is invoked through storytelling and listening. Story sharing is one way to facilitate the transition from ‘Them’ to ‘You’, but it is also dependent on the dialogue about the experiences that ensues. In cases where people may have experienced feeling mistrusted or delegitimised, storytelling becomes particularly important for creating a space of feeling heard and enabling shared experience.49 In the MH ECO example service users, staff and carers first meet separately in focus groups, with peers, to share their experiences and views on areas of change and to prioritise the improvement areas. Here, there is a group of peers who may have had similar experiences of services and dialogue about experience may assist in the creation of the conditions for a relational shift to begin where people can move out of ‘Them’ and into seeing ‘You’, this is made possible because of a shared recognition of our humanity. Similarly, some focus groups might have more of a relation of ‘Us’ at play where the ‘Us’ is used to reinforce group power of experience. Dialogue here may also be critical to shifting any oppositional dynamics for people to recognise and see and hear that they are not alone in their experiences.
Dialogue enables what Arthur Frank calls a ‘moral moment’ to occur which can facilitate or hinder relational transitions from ‘I’ or ‘Them’ to ‘You’. Frank drew on Bakhtin’s concept of a dialogic ethic to capture this moment and bring into focus others.50 In dialogue the ‘moral demand is to grant equal weight to the other’s voice,’ much like Fricker’s notion of epistemic justice, committing to dialogue with people is: ‘more than recognising their inherent dignity and defending their rights; it’s being willing to allow their voice to count as much as yours.’50 The moral moment is when ‘I’ must decide to give equal weight to other cognisant and knowing I’s around ‘[me]’. But in giving that weight there is not a closing off of dialogue. This illustrates how dialogue might be a mechanism for relational transitions from ‘I’ or ‘Them’ to seeing ‘You’. A wider horizon may form in the possibility of seeing one’s self as interconnected, dependent on others and interacting with them to harness capacity for change. This does not gaurantee transition s however our point is that the mechanism of dialogue plays a role in this.
Dialogue might also be said to build what Gabriel called a ‘narrative contract’: the shared agreement between teller and audience of what is possible (meaningful, recognisable and believable). Without shared agreement a story might be challenged on two possible different grounds: by the ‘So What?’ question, which implies that the story fails to carry shared meaning, and by the ‘Did It Really?’ question, which implies that the story fails to carry verisimilitude.51 52 The latter again reinforces how epistemic injustice can come into play once more and how dialogue and recognition are important mechanisms for building narrative contracts that can challenge this.
Cooperative theory
If recognition and dialogue are the basis from which collective identities and narrative contracts can develop within group discussions, then it is possible to suggest that they are mechanisms with a generative function in the movement from ‘You’ to ‘Us’. But those mechanisms require underlying processes and structures of cooperation, accountability and mobilisation to fully bring ‘Us’ relations into being, including shifting the orientation beyond ‘Us’ to ‘We’. To illustrate this from the MH ECO methodology again service users, carers and staff remain separated among peers during the focus group stage. The peer groups enable shared understanding and agreement of experiences to develop which may create the foundations for collective identity formation but, there is equally the possibility that shared experience can be used to reinforce separateness and create a more exclusive and closed off community of ‘Us’ only. For the relational transition to occur from ‘You’ to ‘Us’ to ‘We’ peer groups must necessarily broaden outwards; connections across experiences are important and a new community needs to form otherwise what remains is a closed off moral enclave.
This suggests that mechanisms of cooperation, accountability and mobilisation play a role within relational transitions. As Locock et al concluded from participants recounting their involvement in accelerated EBCD, it was the mutual encounter that left them feeling most energised…codesign offered a space for active partnerships and for revelation and transformation of values to take place.34 In MH ECO the space for new community is facilitated when people move out of the siloed individual storytelling and focus groups stages and into training (or orientation) and shared agreements for codesign activities. At this stage in the MH ECO methodology all three groups finally come together to talk about working in groups and what to expect from the codesign group meetings. This provides the opportunity to start to build the sense that being together can create something new both for individuals and others. There is movement out of shared experiences into shared purposes; the basis of cooperation. As Axelrod and Hamilton noted, ‘cooperation can only take place in situations that contain a mixture of conflicting and complementary interests.’53
Having a transitional space to move from siloed, separated groups to a collective group with shared purpose allows for a sense of commitment to change to emerge. By sharing in common purpose a collective identity forms through what Isaacs and Massey have called the dialogical process, ‘[this] emerges out of and is shaped by our creative engagement with others which often involves the telling of stories to one another.’54 In this collective identity formation, differences are still apparent and the group is by no means homogeneous, but there is agreement around being together and mobilising for change. There is the potential for polyphony as multiple voices come together. The additional element of polyphony is in keeping with the notion of cooperation not as 100% agreement 100% of the time, and draws on Bakhtin’s (1984) portrayal of this as, ‘a multiplicity of independent and unmerged voices and consciousnesses … each with equal rights and its own world [that] combine, but do not merge, into the unity of an event.’55 The emphasis here is on simultaneous interaction and clash, and a dialogic ethic that does not close off the conversation but enables the formation of cooperation through collective identities ‘Us’ and ‘We’. Here it is possible, then, to see that interactions between dialogue, recognition and cooperation.
Creative engagement during orientation processes enables worries and previous negative involvement experiences to dissipate and for a supportive, trusting and safe environment to continue to form. Here, ‘Us’ potentially becomes ‘We’ but it may not be one ‘We’ or everyone involved in ‘We’. The important element of the explanatory theoretical model here is that we see that the cooperative identity in the process of formation sees the possibilities for depending on others in the room for sharing resources. In this regard there is a culture of interdependency that forms around mobilisation for change. Reciprocity and deliberative dialogue are important and they assist to foster collective capacity for change. Identity then becomes the matter of combined values, commitments and beliefs which is not a static nor fixed conception.56
Empowerment and design theories
Mobilisation, then, is a mechanism within group culture that builds on shared purpose becoming a shared commitment. In EBCD and MH ECO, creative and collective capacity for change is brought together by people being supported to make decisions about changes and to codesign solutions to the improvement areas. As Robert and Macdonald have highlighted, Woodman’s notion of organisational creativity emphasises ‘the importance of building creative capacity’ within complex systems.15 The use of ‘what if…?’ kind of codesign activities that take people out of their normal hierarchies and task roles and use their insights and expertise to reimagine a service, as well as the adoption of ‘democratic’ methods inherent to codesign projects, challenge ‘top management… proprietary’ issues and assist in breaking down ‘barriers to creativity’.15 Deciding about changes and working together on these solutions provides an avenue to develop control and ownership, these concepts can facilitate a sense of empowerment. The possibilities here can be expansive but how much they are realised depends on the mechanisms of enactment and creativity; without enactment of change all that is left is ideas.
In the MH ECO methodology the deeper bonds of ‘We’ can be formulated over time through consecutive collaboration and codesign meetings with people taking on different roles in those meetings that afford them other responsibilities and forms of power. These roles enable the development of a feeling or experience that they can be empowered to make a change and enact differences within organisations, but here the enactment must occur too for improvement efforts to be realised. Enactment makes it more likely that people start to see that their efforts will improve things not just for themselves but for others who may come to receive services later. If enactment is not present then the result might be one of disappointment or feeling de-valued since there is a good deal of time and investment of energy required for codesign to occur. In this sense, there is both individual and collective value produced, value might be in the form of greater individual self-confidence or feelings of contribution and speaking up, or recognition of the effect for building better communities and experiences that will be shared by others. Here we can examine the production or otherwise of this drawing both on the concepts of empowerment and design theories.
However, we note that codesign carries a risk that the relational transition to ‘We’ may easily revert back to ‘Them’ or ‘I’ even, as people can lose motivation and faith when improvements are seen to not be implemented. For this reason, the mechanism of attainment is seen to be an important element for the explanatory theoretical model of change. That is, we must be able to identify that people feel a sense that changes will be implemented and that the organisations continue to recognise the importance of their dialogue back to service users and carers about these changes.
Further theoretical advancements for coproduction
It is now timely to pause and reflect back on where this story began. It is indeed plausible for coproduction and associated practices of EBCD to be viewed as a constitutive part of the ‘constant change’, kaizen (continuous improvement), innovation ethic that now dominates in all sectors; a Zeitgeist if you will. In many ways, Raymond Williams’ concept of ‘structure of feeling’ helps us to understand this some more.57 Coined to ‘negotiate the theoretical difficulties involved in bringing together the myriad aspects of cultural change into focus within a signal analysis,’58 structure of feelings referred to:
areas of social experience which are currently being defined (…) a social experience still in process (…) but that has its emergent, connecting and dominant characteristics, indeed its specific hierarchies.59
This structure of feeling represents ‘a mood or way of thinking discernible retrospectively across the entire socio-cultural and political spectrum at any given time.’60 Coproduction is a socially deliberative process, and such a process is inevitably relational and emotional (or ‘affective’) because participants need to pay attention to new people, new interactions and new ideas.60 This new structure of feeling brings with it relational opportunities and challenges for exploration.
The ability to codesign with others and produce workable futures confirms social and organisational relevance and shapes ways of going on that are ‘more or less’ democratically developed. Yet, the tension persists, between contextual economic and political conditions within which coproduction efforts may arise and the desirable outcomes of equality, democracy and empowerment. Balancing the needs of participants with realistic goals is important, recognising that for some private benefit motivates more than public good, and that some coproduction efforts are driven more by scarcity of resources and dwindling publicly funded services. These contextual drivers are important to acknowledge, they shape the relational space within which people come together and the organisational contexts within which coproduction efforts are occurring. So far these contextual factors have not been accounted for in the description of the explanatory theoretical model but it is acknowledged that this will play a role in the considerations and evaluations of how the relational worlds are enacted within codesign.
It is important to re-emphasise here that the explanatory theoretical model brings together mechanisms and transitions that have been identified as important for the MH ECO model. Such mechanisms and transitions have been noted within other studies utilising coproduction and EBCD but there is further work to be done to advance this theoretical model according to those studies. A detailed explanatory theoretical model advances the field in the ability to understand and explore what does and does not work in coproduction in the relational spaces within which efforts occur and to develop ways to attend to enhance the things that do and those that do not. More importantly it offers the potential to understand why. We have acknowledged in the descriptions of the transitions that there is the possibility for an ‘I’ and ‘Them’ process to remain at work, peers (both people with lived experience and staff) can reinforce negative thinking and experiences, and power dynamics and hierarchies of organisations can be reinstated in ways that close off the opportunities for transitions. There may be contextual factors that limit possible transitions and these must be considered in any given exploration. We have also noted that people might begin from a starting point of Us or We orientations and not solely be isolated and separated.
The explanatory theoretical model presented illustrates that coproduction efforts seek to go well beyond the collaborative design of practical solutions. Practical solutions are important and indeed they are part of the goal of collective efforts, but they represent something else that is of even greater significance: the acquisition by service users, carers and staff of the ability to negotiate (more or less) mutually acceptable ways of going forward into the future, and knowing that all present have helped shape that future. For this reason, the implementation of those practical solutions is an equally important topic, but one that cannot be addressed within the current remit of this paper. Admittedly, and on the one hand, this process entangles codesign participants in what Sloterdijk has referred to as a spiralling demand for dialogic and inventive competencies.61 On the other hand, however, Sloterdijk is clear about codesign bestowing on participants a sense of being able to ‘simulate sovereignty’ over their future confirming the positive and productive aspects of their relationships and activities.61 This may have a generative effect of positive interpersonal and portable experiences, but without attendance to the contextual and environmental forces that shape these practices and a commitment to transformation of these within coproduction and codesign efforts, there is a risk that sovereignty becomes mere rhetoric. Indeed, within the complexities of mental health and overall involvement in service improvements, sovereignty is not merely transferred by virtue of participation.
This latter point explains why codesign as situated coproduction of a shared future may have significant implications for service users, carers and staff well-being, but one that exists in tension. Their future (or at least aspects of it) has been collectively sketched out, they have all had some possible role in this planning and the sharing of the planning yields some degree of confidence in the plans having legitimacy; playing a role in this planning confers that legitimacy on to me (‘I’) as individual participating stakeholder, and seeing the plans being realised provides the final confirmation of that legitimacy (‘We’). The extent of how transformative this realisation is must by the focus of future theorisation efforts in the field.
It is now also possible to envisage the significance of these participatory endeavours for healthcare in general, and for healthcare redesign and systems reform in particular. Both are complex endeavours. For that reason, a brief digression is warranted into how the complexity of healthcare as a system has been construed. Where ‘complexity science’ favours a ‘view from nowhere’62 that sees phenomena as objectifiable with the aim to depict the totality of healthcare from a safe distance, codesign theory accepts that healthcare complexity manifests for staff and service users where care happens; in the here and now. Codesign theory accepts that the here and now is empirically complex thanks to past management decisions, design choices, technological complications, human affordances, spatial constraints and circumstantial specifics, and this might carry forward into the future. In that sense, codesign aligns with Giddens’ view of the ‘structuration’ of the here and now—a dynamic implicating local actors, pasts, resources and potentials.63 64 Giddens’ perspective has been integrated since into ‘practice theory’65 emphasising how humans ongoingly perform the here and now into existence (cf Butler’s notion of ‘performativity’).66 However, the general point remains of relevance to how we conceive of healthcare complexity, of how clinicians and service users are caught up in complexity. For codesign, complexity manifests itself not in some abstract system elsewhere, but in the immediacy of the here and now, imposing tasks and challenges.
Conclusion
Ultimately then, processes of coproduction (and related but distinct practices such as EBCD, cocreation and coinnovation) embody and propose solutions to here-and-now complexity but one that is connected to past experiences that must be shaped into new prospective futures. Participation itself engages local stakeholders in apprehending complexity as empirical reality, and in sketching out ways of going forward amidst uncertainty, it does not mean that everyone is on equal footing or in agreement; but to get closer to this ideal the field of coproduction, as others have acknowledged,1 2 needs to have better identification, detail and understanding of the underlying mechanisms (those process, entities and structures) that might facilitate the conditions for this. Codesign accepts the limits that apply to local actors’ knowledge and decisions, but takes heart from the practical benefits and legitimacy generated through multistakeholder dialogue, respectfully achieved conclusions and feasible initiatives. Codesign thus embodies a uniquely pragmatic and humble stance: various scenarios may be sketched out appearing equally feasible67; no scenario, decision or outcome is likely to be optimal, and scenarios, decisions and outcomes remain open for redesign and renegotiation in the future.
Codesign is now a general competence that is beginning to spread from organisations who focus on engaging service users and professional front line teams and their leaders in cocreated changes, into everyday practices of our sociocultural and political life. In this regard, codesign engenders opportunities for citizens to become part of ‘how we go on’68 within the moral era of medicine. If this third era is one that is characterised by increasing levels of participation then an explanatory theoretical model of change that can critically evaluate coproduction efforts is important, if not essential In many respects, the new Zeitgeist signals to a collective spirit in the face of a highly individualised, competitive sociocultural landscape but as other authors have noted this is not without complications and cautions. Is this movement of participation any different from cooperative practices we have seen in the past we ask? For example, the Mondragon cooperative social system in the Basque region of Spain emerged directly from the needs of the populace for welfare, education and economy to cocreate their own structures and systems but, as quickly as the social system formed it too fell prey to greater economic and political forces transforming into a corporation. The lesson is one about the question of value and the looming possibilities of economic capture.
Acknowledgments
In addition to the authors listed, the CORE study is dependent on the commitment provided by non-government and community health centre providers of mental health services as partners in the project. The study team acknowledge the support of the staff, service users and carers of these organisations and the ongoing work of the Victorian Mental Illness Awareness Council (VMIAC) and TANDEM representing Victorian mental health carers in their development of the original Mental Health Experience Co-design methodology (MH ECO). The authors acknowledge the research support of Kali Godbee (study coordinator), Roxanne Kritharidis (intervention coordinator), Konstancja Densley (data manager) and Dr Patty Chondros (lead biostastician).
References
Footnotes
Twitter @VictoriaJPalmer
Contributors VJP conceived the larger CORE study in conjunction with staff located in community mental health services. VJP, WW, RC and HH workshopped the activities of MH ECO to identify preliminary mechanisms of change. GR, RI, JG, JF, DP and LR reviewed and contributed to the refinement of these. VJP, WW and RC led the development of the explanatory theoretical model with expansion from RI, GR, LM, HB and HH. All named authors participated in the preparation of the manuscript, providing written comments on drafts and approving the final version.
Funding The CORE study was funded by the Mental Illness Research Fund and the Psychiatric Illness and Intellectual Disability Donations Trust Fund (MIRF 28). The Mental Illness Research Fund aims to support collaborative research into mental illness that may lead to better treatment and recovery outcomes for Victorians with mental illness and their families and carers.
Competing interests None declared.
Patient consent Not required.
Ethics approval The University of Melbourne Human Research Ethics Committee (HREC No 1340299.1-12) has approved this study. The Federal Government Department of Health has approved the collection of Medicare and Pharmaceutical Benefits Scheme data and the State Government of Victoria has approved the collection of hospital admission and triage data.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Unpublished data are available from the study related to action plans and improvement areas and codesign process evaluation work. Data requests are considered on a case-by-case basis and must include ethics approvals.