Article Text

Abstract
The history of paediatrics and child health is increasingly recognised to be about children themselves and how they and their families cope and adapt to their medical condition rather than about medical practitioners and august institutions. This article considers two case studies, showing how two Georgian fathers cared for their children when sickness struck and their reactions when the children died. Davies (Giddy) Gilbert, FRS (1767–1840), was a member of Parliament first for Helston and later for Bodmin. (He married Ann Mary Gilbert in 1808 and formally changed his name to Gilbert; the change received royal approbation in January 1817.) Gilbert recorded the birth and development of his son Charles (1810–1813), in one of the very earliest developmental chronicles. He regularly recorded his child’s progress, including height, weight, social interaction, communication skills and speech. Apparently in good health for most of his life, Charles developed an acute abdominal disorder and died unexpectedly. John Tremayne (1780–1851) was a member of Parliament for Cornwall. His son Harry (1814–1823) had increasing bilious attacks, headaches and a squint from the age of 6 years, and died despite the best medical advice available. Current medical opinion would presume an intracranial tumour. Tremayne graphically expressed his pain as he closely observed his son suffer, apparently as much from the treatments as from the disease itself. This study sheds light on clinical aspects of Georgian medical practice, the medical marketplace and the nature of relationships between these fathers and their children.
Statistics from Altmetric.com
Perceptions of 19-century fatherhood were explored by late-Victorian writers including Anthony Trollope and Samuel Butler. In Phineas Finn, Trollope relates a conversation between a grandfather and young child: “Papa is very well, but he almost never comes home,” and further, “Your papa is a busy useful man, and can’t afford time to play with a little boy as I can.”1 In The way of all flesh, initially drafted in the 1870s, Butler wrote, “Yet, when a man is very fond of his money it is not easy for him at all times to be very fond of his children also. The two are like God and Mammon. … His money was never naughty, his money never made noise or litter, and did not spill things on the tablecloth at meal times, or leave the door open when it went out,” finally opining that “It must be remembered that at the beginning of the 19th-century the relationships between parent and child were still far from satisfactory.”2 These comments from an eminent Victorian writer of unsatisfactory child/parent relationships in earlier times only reinforces modern stereotyped perceptions of the past that relationships between parent and child were “cold”. Such a perception was rarely questioned by historians until the 1980s.
However, historians such as Linda Pollock, Ralph Houlbrooke and Rosemary O’Day have disputed such a proposition, although Lawrence Stone has argued that there was only so much “emotional capital” and accordingly there was limited expressed affection for the child that could not live long. Interestingly, Mrs Thrale, on the death of her eighth child in 1772 only 10 hours after birth, wrote in her diary: “poor little Maid! one cannot grieve after her much and I have just now other things to think of—this has been a sad Lying In”.3 However, modern scholarship presents a more complex, evolving and varied picture. While Davidoff and Hall explored the evolution of “separation of spheres”4 in which the gender balance evolved between 1780 and 1850 as the separation between the work place and home increased, Tosh specifically contends that “the experience of fatherhood was highly varied—and certainly not be contained within any stereotype image of “the Victorian Father”.”5 Critically, as late as 2003 Lisa Smith argued that “historians have not taken much interest in the family’s role in medical care”.6 Appropriately, therefore, this paper seeks to demonstrate the capacity of two late Georgian fathers to care for their sick children with great diligence and, in these specific cases, suffer emotionally in the process.
Although medical practice is based upon obtaining a clear patient history, many historians question the value of “stories”, anecdotes or what Anne Digby refers to as “history from below”,7 as such evidence may not give a coherent account of the past. Will Coster, in his study of family and kinship, concurs, suggesting that history based on such anecdotal evidence “tells us nothing about the frequency of circumstances or the nature of social change”.8 Yet medical practitioners, and increasingly many historians, recognise the value of micro-histories to reconstruct, or record, the “voice” of an individual. Specifically, L M Beier, when referring to the diary of Ralph Josselin, written between 1641 and 1683, suggests that “such records of unique, personal experience are invaluable to the historians, providing as they literally do, a voice from the grave which can make the past live as no other source can”.9 The authors believe that such “voices from the grave” are critical in enlightening our understanding of the past; the two case studies reviewed below improve our understanding of the effect of sickness and death on the immediate family, and the father in particular.
CHARLES GIDDY (1810–1813)
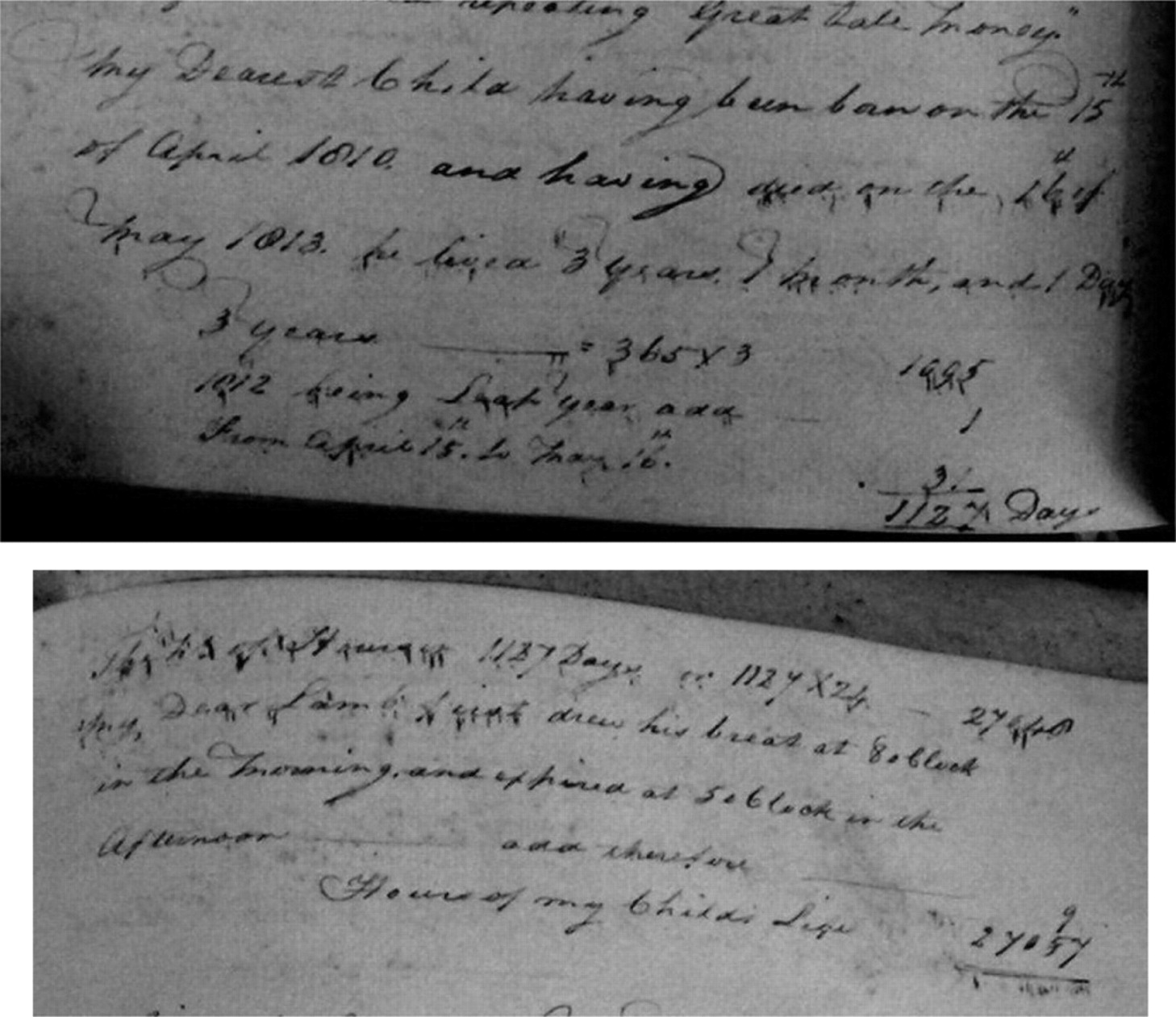
Charles Giddy’s father was the eminent scientist Davies Gilbert FRS, MP (1767–1840) (fig 1), who later became president of the Royal Society. This case study is taken from a memorandum written in December 1813, after Charles’s death at the age of just 3 years and 1 month. The memorandum was based on entries taken from Davies Gilbert’s “Almanacs”, or diaries. The language is therefore coloured by the anticipation of the tragedy that was to unfold.

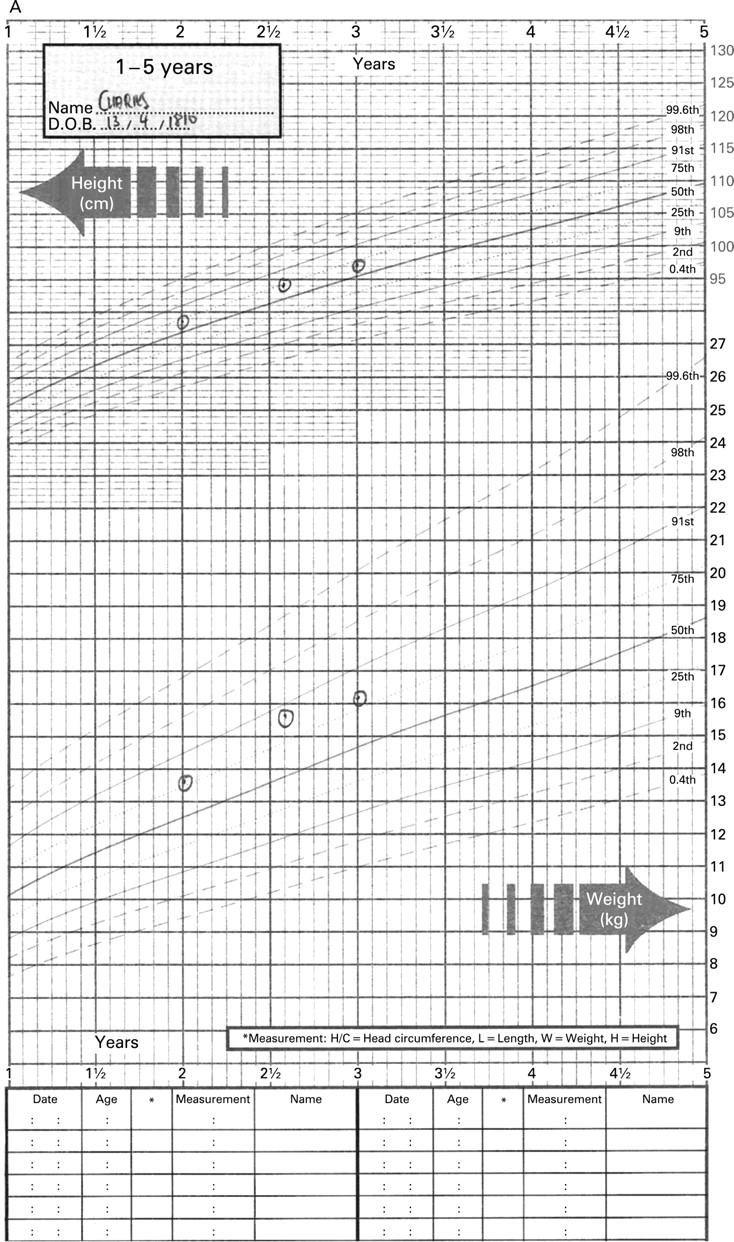
Pertinent to this study are the observations that Gilbert made of his son’s height, weight, behaviours and reactions to people, materials, noise and toys (table 1). Considering his described physical attributes on a 21st-century height and weight chart, during his first year of life Charles’s weight gradually increased from the 50th to the 91st centile and then in the second year generally followed along or above the 75th centile (fig 2A, B). The three recorded Figures 2B and 2A will be transposed to appear in the right order. height readings are from the second year onwards, and they too generally follow under the 75th centile for a child born today. Gilbert’s own height can be extrapolated from his comments written on 13 April 1812, Charles’s second birthday: “Charles weighed 30 lbs and measured 2 ft–10¾ in, just ½ my height.” Gilbert’s height was 176.53 cm, on the 50th centile of present-day adult height. Although there is a slight drop in the centile values for the child’s last reading for both height and weight, neither of these would cause immediate concern to a present-day paediatrician or other child healthcare professional,10 although one would be interested in reviewing the situation 6 months later, before deciding whether any further action was warranted. This paediatric coauthor (ANW) does not believe they are of any significance or relevance in terms of predicting Charles’s ultimate demise. Stature is only one of several biological markers of nutritional status, but there is a long tradition of using stature to assess health aspects of human welfare.


In Britain, Floud and Harris demonstrated that the mean height for an adolescent born in the late 1950s was more than 11.42 inches taller than those born in the mid 18th century, with a sustained increase in average male heights from 1850 onwards. So Gilbert’s height, which would place him on the 50th centile today for an adult, would certainly have made him relatively taller in the early 19th century when compared with his peer group. However, this anthropological analysis was extracted from military records.11 12
Comparable data for growing children of the very early 19th century do not exist. It was clear from these records that Charles Giddy was well nourished. Buchan, when describing rickets in 1798, mentions that “bad nursing is the chief cause of this disease. When the nurse is either diseased or has not enough milk to nourish the child it cannot thrive.”13 It was only from 1828 that Villermé recognised the stunted growth and the multitude of interacting factors that contributed to the excess mortality and morbidity of children from poorer backgrounds.14
Box 1 Charles Giddy postmortem report
Hollis Street May 17th 1813
Medical Inspection of Charles Davies Giddy Aged three Years.
The Body was not emaciated, the Death had taken place about twenty four hours before this examination. On opening the Abdomen a serous opaque fluid issued which was obviously the consequences of inflammation. The Peritoneum was extensively loaded with inflammatory coagulated lymph and in parts with Pus, the small intestine were highly inflamed through a great part of their length these appearances decidedly account for the fatal event. It may be worthy of notice in Mr Giddy’s Family that this Child had a disordered state of the absorbent Glands of the Mesentery, which may lead to future precautions in the Management of the Health of the other Children.
Signed,
Edward Ash MD Ch. Combe MD
Anthony Carlisle S T. Knight S
At 7 weeks Charles was vaccinated “and went through the disease in the most perfect manner, and evidently without inconvenience”.15 On 10 September 1810, when 21 weeks old, “Charles weighed 17lbs [7.73 kg] which gives a rate of increase of an ounce a day.” (Paediatricians, including one of the authors (ANW), still use the yardstick of healthy weight gain of an ounce every day except Sundays, or six ounces a week.)
At 28 weeks, “if Charles were held against a looking glass he immediately turned his head away and continually in whatever position he was placed.”16 On 10 November, at 30 weeks, he “had cut his first tooth without any suffering”.
At 1 year, Charles “returned the ball to me several times with a pretty good general direction”,17 and when shown a picture of his father, “he kept turning his eyes from me to the Picture and back again several times.”18 By the time Charles was 30 months old, he was regularly playing out of doors. While out walking on one of his childhood haunts, his father observed that “Charles must be stronger at a younger Period”19 than he himself had been at that age. Two days later, during harvesting, Charles “was almost the whole day with the men bringing in our Barley”.20 Physical development brought with it a streak of obstinacy, and Davies Gilbert’s wife occasionally used a “little rod” to chastise their son, which is unacceptable by present-day standards.
However, Charles’s developmental progress was not smooth. He demonstrated delayed expressive language development, good compensatory use of non-verbal communication, delayed oro-motor skills, feeding and speech, and reasonably good verbal comprehension.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Final illness
A month after his third birthday, 14 May 1813, Charles had been running up and down stairs and appeared in very good health. However, after dinner he told his mother that he did not feel well. He went to bed and soon fell asleep, although he was rather restless. The next morning Peggy, a servant, brought Charles into his parents’ bedroom, suggesting there was not much wrong with him, as he had “eaten two Cupfuls of Bread and Milk”.21 After breakfast he was still unwell and was given two grains of calomel, which he took willingly, saying, “Papa give T(Ch)arley something to make T(Ch)arley well.”21 He then vomited and his parents thought that the cause was the mackerel he had eaten the previous day, which had also upset one of the servants. Accordingly, Gilbert refrained from giving Charles any further medication and left the house on business. On his return home, he was informed that Charles had remained drowsy but had displayed no other symptoms. As Charles had had no bowel movement, Gilbert was about to direct another dose of calomel when it was suggested by Mrs Gilbert that in the past, two grains of James’s Powders had been effective, and this medicine was given, “supposing there might be a little fever, his pulse were rather low but quick”.21 The following day he was hot and restless, with no bowel movement. He was given senna tea, but he produced some bile and was given a further two grains of calomel. His tongue appeared foul and Dr Combe was called. The doctor thought little of the symptoms, directed that an enema be given, which was dealt with by his mother, and said that he would call again later that day. Gilbert, whose “mind was entirely easy”,22 again left the house on business. Thereafter, Charles’s mother and aunt sat by his bedside, where he kept asking for water, which he was given. He asked to make water but passed very little urine. He was then about to be given another enema but he protested to his mother, “Mamma no ma”,22 and while she was with him she noticed that his pupils were dilated. To her, such a sign meant that he had “water on the brain”. Paediatricians would recognise such a condition as an imminent pre-terminal event. Mrs Gilbert quickly wrote a note to Dr Combe and ordered the servants to bring a tub of hot water to the nursery while her sister ran for a Dr Ash, who also attended the dying boy. The warm water was applied to the small boy’s body but in vain.
Shortly thereafter Charles quietly expired. It was 16 May 1813.
Returning to the house an hour later, Gilbert found his father and sister in tears, although no immediate reference was made to his wife’s reactions. Gilbert writes a great deal about the family’s reaction to the sudden death of such an apparently healthy and much cherished little boy just 3 years old. Pertinently, he perceives his own reaction as beyond expression: “I rushed into the room, embraced the Dear little Body—called loudly on my Dear Charles—I then threw myself on a Bed where I remained for a considerable time with my mouth wide open making such inarticulate sounds as I never remember to have heard. This kind of paroxysm continued at intervals during all the days I remained in London and broke out with peculiar strength each time I woke during the night.”22 Subsequently, Gilbert made an illuminating comment related to the family’s reactions to such a tragedy and his relationship with his son. “His Mamma, Grand Papa, Aunt and Uncle Guillimard all suffered extremely but no one in an equal degree with myself. His Mamma probably loved Charles with an equal degree of natural affection but I had entwined with mine a thousand circumstances of Interest and endearment.”22
Gilbert had a postmortem examination undertaken. This is a procedure that, then and now, parents are generally reluctant to have performed upon their children’s bodies. Gilbert’s insistence was surely driven as a balm to partially assuage his intense grief and assure him that his son could not have been saved. There is little contemporary material on postmortem examinations upon children at this time, which today are subject to a rigorous scrutiny. The period of Charles’s death was at a time before Thomas Wakley’s drive to reform the coroner’s system in the 1830s and the passing of the Anatomy Act of 1832.23
The postmortem concluded that “this Child had a disordered state of the absorbent glands of the Mesentery, which may lead to future precautions of the Management of the Health of the other Children.”24 (Box 1)
It is difficult to be sure what was the cause of Charles’s symptoms, leading to peritonitis and his death. There is no evidence of intussusception, obstruction, volvulus, bowel infarction or bowel perforation due to the enemata that he had received. An appendicitis, however, particularly classically a retrocaecal appendicitis, could explain the lack of typical features demonstrated by Charles, such as lack of guarding and lack of percussive tenderness. Indeed, in a recent large case series, 44 per cent of paediatric patients with appendicitis presented with six or more atypical features.25 Given the “disordered state of the absorbent Glands of the Mesentery”, tuberculosis needs to be considered, but it should be borne in mind that Charles was previously well.
The swollen small bowel does also suggest the possibility of typhoid, but gastrointestinal symptoms tend to occur in the second stage, after a longer period than Charles was unwell for.26 Finally, with a servant also being made unwell through ingestion of mackerel, scombroid needs to be considered. However, this disease, which is caused by excessive histamine release from mackerel and tuna, is self-limiting and usually subsides within 24 hours.27
What is most striking to healthcare professionals and those who have experienced death at close quarters in their own lives is not that such extreme expressions of misery occurred but rather that Gilbert wrote it down in such detail. He most poignantly even wrote his calculation of how long Charles was alive, in days (1127) and even in hours (27 057) (fig 3).
Any reader cannot fail to be moved by the father’s anguish.
HARRY TREMAYNE (1814–1823)
The second study is taken from letters written by John Tremayne (1780–1851) to his father between 1820 and 1823 relating to his son Harry’s increasing indisposition from the age of 6 years until his death at age 9. In January 1821, Harry had “a violent attack of bilious sickness”.28 The medicine he was given proved ineffective and his father feared that “the tendency to hiccups will continue.”29 Harry seemed to have improved and Tremayne wrote to his father that “little fellows are soon down & soon up.”30 Later, when writing from London, Tremayne became convinced that the cause of Harry’s stomach attack had been the result of “the stinking fog & unwholesome Air”.31 One day in February, Harry’s sickness had returned and he brought up his dinner undigested. Tremayne remained convinced that Harry’s digestive condition was due to his being in London, his condition specifically being “produced by the state of the atmosphere, which was so thick, that it was dangerous to walk the streets almost & every body complained of being sick by it”.32 However, he called in the eminent physician Dr Maton (1774–1835), a royal appointee. Maton opined that Harry’s parents “be quite easy that there is no Organic Defect but that is a mere irritation of the Stomach or upper intestines, against which during the interval of the Attacks every thing must be done that can be towards strengthening the Stomach, by which time he will get over it—We cannot think of any particular Cause to which to attribute these Attacks.”33 Nonetheless, Dr Maton prescribed “something to strengthen the stomach & at the same time a Powder to stimulate his Digestion”.34
As the attacks continued, Tremayne then called for a second opinion from the eminent Dr Matthew Baillie (1761–1823), a royal appointee since 1810, who had attended George III during his final illness. He was a nephew of the celebrated William Hunter (1718–1783). Neither doctor could think of any particular cause for Harry’s condition, while Dr Baillie agreed “with all who have seen him that there is nothing wrong with his internal structure”.35 However, in March Dr Baillie suggested that young Harry might have an inherently weak stomach.35 The attacks continued and by April these two eminent physicians were visiting Harry weekly. After one serious bilious attack, which Dr Baillie believed was due to mucus in his stomach, he was given an emetic. The regularity of the attacks increased and then Tremayne mentions “a turn in his eye which they [Baillie and Maton] are inclined to believe is entirely from sympathy with the stomach but now as a precaution they have ordered 6 leaches lest it should be connected with the head”.36 Harry’s condition deteriorated further and he was treated with a blister on his back, which “was followed by a most profuse and violent perspiration continuing the whole of the day yesterday and even a part of last night”.37 Tremayne, having reluctantly accepted such treatments, wrote to his father that “The thing I lay hold of and cannot give up is that the reachings are attended with violent Headache which rebates as the stomach empties and ceases when it is quite clear”.37 Shortly thereafter, Maton suggested that the cause of the problem was the head, and Baillie concurred. Baillie’s opinion was recorded verbatim: “if it is a stomach affection I am sorry for the boy being ill, but I feel no harm—if there is a tendency to pressure on the optic nerve, which I am of the opinion there is, it is a thing to be guarded against in every possible way as leading to the most fatal result.”38 Initially, Tremayne appears to have been ambivalent regarding the seriousness of the squint, still believing that the source of the problem was the stomach. He commented about “that very distressing Turn, which if it only disfigures him, is comparatively trifling—if it is a sign of anything else, it is too frightful to think of!!”39 Tremayne informed his father of the various treatments Harry was given, including various applications and blisters with their attendant debilitating effects of pain, irritation and sleeplessness. While we may pity Harry for the suffering he endured from such ineffective treatments, Tremayne’s own deep concerns relating to such treatments were clear when he wrote that “the Effects of the Blister is excessive”.40
By now Harry was clearly demonstrating hard neurological signs. On 20 June 1821, Tremayne consulted Alexander, an oculist, who diagnosed a weakness in one of the muscles of the eye, “by which the balance is destroyed”.41 Sadly, no further information is available concerning this medical practitioner. Later, when the family were visiting the West Country, Tremayne wrote, “Poor fellow! His strange gait and tottering unsteady action induced me to desire Astley Cooper to look at him before we left town—and I am sorry he gives us little Comfort about him. He says he will require most minute Care and Attention to prevent deterioration of Blood, which certainly exists in the head having the worst effects—at the same time his overloaded mind and active spirits are good symptoms—but it is idle to conceal from one’s self the fact that he has great fears for him.”42
Early in 1822, Harry’s condition improved a little and the family were staying in Launceston when his attacks returned together with an infection of the throat and chest. During this time, Tremayne wrote no fewer than 27 informative letters to his father in six weeks. From this correspondence two factors emerge. First, Harry’s condition was such that Tremayne was unable to move the family back to London and, second, that he suffered emotionally as he cared physically for his son. On 4 March 1822, he wrote to his father that “We had intended to go tomorrow but on taking Harry out in my Arms in the Garden to day I found he bore it so badly, that we have been obliged to give it up. I am now almost in despair of ever moving him.”43 A few weeks later Tremayne wrote that a Dr Lake had prescribed “some preparation of Antimony, I think, for which it will be necessary to have his Head shaved and as it will occasion some irritation of the skin, I am doubtful how he will bear it, especially as any thing on the Head or about it annoys him considerably.”44 Less than a week later the father’s fears proved well founded: “I found on my return last night that Harry had been suffering much from the Application to his Head, which has deprived him of rest and given him much fever and irritation.”45 In due course Harry became totally blind and continued to deteriorate despite all the efforts of many doctors and his father’s care. He died in March 1823.
Harry probably had a low-grade intracranial tumour. This would lead to raised intracranial pressure, and in combination with possible focal effects of the tumour, effects on neighbouring neural structures.46 We can speculate that this could have been a meningioma, a craniopharyngioma or even an optic nerve glioma, but the absence of a postmortem examination makes it impossible to say more. (No concerns were raised about Harry’s growth, which may be an argument against a craniopharyngioma.)
Dropsy of the brain was recognised in the early 19th century. William Buchan, in Domestic Medicine, lists “scirrhous tumours or excrescences within the skull” as one of many causes. Buchan recognises its initial symptoms of “pain in the crown of the head, or over his eyes; he shuns the light; is sick, and sometimes vomits; his pulse is irregular and generally low: though he seems heavy and dull, yet he does not sleep; he is sometimes delirious, and frequently sees objects double: towards the end of the disease, the pulse becomes more frequent, the pupils are generally dilated, the cheeks flushed, the patient becomes comatose, and convulsions ensue.”47 Buchan, sadly, gives a grim prognosis but encourages treatment: “No medicine has hitherto been found to carry off a dropsy of the brain. It is laudable, however to make some attempts, as time or chance, may bring many things to light, of which at present we have no idea.” Buchan recommends purges as well as blistering-plasters applied to the neck or back part of the head. He comments that he has never seen a cure, “but in so desperate a malady everything deserves a trial”.47 His appendix relates that the often late presentation of these children makes it “too far advanced to admit of a remedy”. Although he feels that with an earlier presentation “something might be done”, he cautions that “these symptoms are not yet sufficiently known, and are often mistaken even by physicians themselves”, relating the case seen by another doctor “who had all along mistaken this case for teething”.47
In the 21st century, late diagnosis of intracranial pathology remains a significant paediatric problem. Clinicians must always be mindful to consider this differential diagnosis if intracranial tumours are to be discovered through the appropriate medical imaging. Indeed, a recent review of 200 cases of childhood brain tumours revealed that a prolonged symptom interval is associated with low-grade tumours and age over 3 years, which would fit Harry’s case history.48
But in what manner do these two case studies enlighten our general understanding of the late Georgian medical landscape?
THE LATE GEORGIAN MEDICAL MARKETPLACE
The medical marketplace in the early 19th century had developed since the mid 18th century with increasing specialisation and professionalisation. Central government was just beginning the long road to central control with the Apothecaries Act of 1815. Nonetheless, this marketplace remained like any other market, a case of supply and demand, Burke and Porter commenting that “medicine—despite the genteel pretensions of its upper echelons—was essentially determined by market forces.”49 Yet this contemporary market was in a state of flux, initially suffering some over the supply of practitioners after the end of the Napoleonic Wars, while “Growth in demand in what was still a consumer market was fuelled by an expanding and increasingly well-to-do middling class as well as from greater medical expenditure under the Old Poor Law.”50
Pertinently, Tremayne’s need to travel between London and his Cornish constituency before the advent of the railways demanded accommodation in places where he would normally have had no need to seek medical help. Significantly, the first reference of Harry’s indisposition was in Honiton in 1821, when Tremayne wrote to his father that “I was really unwilling to launch into the New Road where I knew of no Physicians, whereas I knew there was a good one here & at Salisbury.”51 Accordingly, apart from consulting such eminent London physicians as Maton and Bailey, Tremayne would have been obliged to seek help for Harry from practitioners in various locations between London and Cornwall. On occasion, Tremayne was unable to continue his journey because of Harry’s increasing debility. In such circumstances, he endeavoured to base the choice of practitioner on reputation, either from his family, specifically his father-in-law in the case of Fowler from Salisbury, or one “whose reputation stands high with the London surgeons”,52 in the case of Barnes from Exeter. He consulted the celebrated Astley Cooper when visiting Bath, where he also had the prescriptions of other physicians checked, as occurred, for example, in relation to his wife’s physician.53
What Tremayne’s experiences imply is that the medical marketplace of the 1820s was well supplied with practitioners over a wide geographical area and that reputations were important. Despite the competitive nature of the contemporary market, there was a general level of respect between practitioners. Specifically, there appears to have been acquiescence to patients’ obtaining second and third opinions as well as having practitioner’s prescriptions and treatments checked by other practitioners. Notably, such eminent physicians as Baillie and Maton consulted together when jointly caring for the young son of a member of Parliament.
PARENT–PRACTITIONER RELATIONSHIPS
Both these Georgian gentlemen were affluent members of Parliament—Gilbert, a leading scientist, and Tremayne, from an ancient landed family. The attitude of both fathers, who were clearly able to afford medical consultation when they deemed it necessary, was noteworthy.
Gilbert rarely called a doctor until just before his son’s death, yet Tremayne was in constant communication with a number of practitioners, 13 being mentioned by name from various locations from London to the West Country.
Although Gilbert’s experience of doctors during his son’s short illness was limited, he appeared to have faith in the medical fraternity of the day. He allowed his son to be inoculated when just 7 weeks old and, further, having insisted that a postmortem be carried out, he must have had some solace when the doctors convinced him that nothing could have saved his son.
While Tremayne’s doctors tried every treatment at their disposal to save Harry, Tremayne watched their efforts in despair. Yet on at least one occasion he defended the practitioner’s care of young Harry against his father’s criticism. Nonetheless, he kept his father fully informed, even when it exposed his own emotional suffering. On 1 May 1821, he wrote to his father: “so they are going to apply leaches again to his temples and to continue medicine … The Blister is to be kept open at least in part. I am satisfied with this however painful to my feelings as in the nature of an insurance against the greater [good].”38
The evidence strongly suggests that both these gentlemen had faith in the medical practitioners they consulted, even going so far, in Tremayne’s case, as to defend them against criticism.
TWO GEORGIAN FATHERS’ ABILITY TO CARE AND THEIR PROPENSITY TO SUFFER
The evidence suggests that both fathers took charge of their son’s care, even if aided by spouse, family and servants. Both questioned, but accepted, the medical advice received and both took a major part in physically caring for their child.
While Gilbert suffered acutely from the shock of the sudden loss of 3-year-old Charles, Tremayne had closely observed Harry suffer greatly over a 3-year period, probably more from the treatments than the disease. While Tremayne had apparently come to terms with the inevitable loss of his son, Gilbert was profoundly shaken.
There are elements within the human condition that are timeless. This article reaffirms the effect of illness on the family from an early-19th-century perspective. Ultimately, these case histories concern the ties that bind. In 1517, Sir Thomas More declared to his daughter that “Nature in her wisdom has attached the parent to the child and bound them together with a Herculean knot.”54 For these fathers, we can see how this knot held when their children experienced disease and premature death.
These two fathers, as members of Parliament from the West Country during a similar period, would inevitably have been professionally acquainted. Additionally, they also appear to have been personally well acquainted, Tremayne having attended the baptism of Charles Giddy in May 1810. To what extent these two Georgian gentleman were atypical in their responses to the birth, sickness and loss of a young child is not currently adequately researched or appreciated.
MODERN UNDERSTANDING OF EARLY-19TH-CENTURY CHILD CARE
The developmental histories, of course, are not comprehensive. It should be recalled that there was little if any understanding of paediatric development, and there were very few contemporary histories. Illingworth notes, “Teidemann in Germany (1787) was the first to publish a detailed record of the development of one child, but it was not until Charles Darwin published … that interest was aroused.”55 Charles Darwin was inspired just before his engagement in 1838 by the idea of writing the Natural history of babies and started to keep diaries of his children’s development from the birth of his firstborn, William, on 27 December 1839. However, Darwin’s material was published only much later, in On the expression of the emotions in man and animals (1872) and A biographical sketch of an infant (1877).56 Other developmental histories, based on a more systematic foundation, by Preyer (1882)57 and Shinn (1893)58 followed, although all suffered from the subjective nature of their observations and later concerns about observer bias.
These case histories were written before the first scientific understanding of child development. Nonetheless, Gilbert’s observations of his son were systematic. The voices of the child are hardly heard during their sickness but the vivid descriptions leave little to the imagination. We encounter two fathers of the late Georgian period, both in deep distress because of the suffering and death of their children. Whereas no record of Tremayne’s expressions of grief after Harry’s death have been found, Gilbert’s comments some seven months after the death of Charles are profound: “Best Hopes, the kindest Gift of their Fabled Benefactor to Mankind is torn from my Brest, each pleasure arising from the sweetest source is now dashed with pain, and the Temperament of my Mind has undergone a lasting change.”59
From the modern perspective, we see the value of paediatric palliative care, which rightly is now playing an increasingly important role. Finally, these case histories also demonstrate that parents living with the hard facts of the sickness, treatments and death of a child also require care and support.
Acknowledgments
We would like to thank Dr Margaret Holloway, Dr Mark Hunter, Dr Wendy Kagen, Dr Phyllis Preston, Dr Jonathan Reinarz, Mrs Georgina Slater and Dr Robert Sunderland for their comments, and the staff at the Cripps Postgraduate Medical Centre, Northampton General Hospital, and Oxford Brookes University for their support. We also thank the Cornwall Record Office, Truro, and The Cornish Studies Library, Redruth.
Supplementary materials
web only appendix 34/2/70
Files in this Data Supplement:
Footnotes
▸ A fuller version of Gilbert’s observations concerning his son is available at http://mh.bmj.com/content/vol34/issue2
Competing interests: None declared.