Article Text

Abstract
Should medical humanities become part of the core curriculum in medicine? This paper describes the experiences of one medical school that decided it should. The paper describes the professional and academic rationale for this decision, the process by which it was implemented, the structure of the course, the strategies for assessment of students' work and the results of a teacher evaluation.
- Medical humanities
- medical curriculum
- medical education
Statistics from Altmetric.com
Author's note: This is one of a linked pair of articles about making medical humanities a core part of the medical curriculum. The other paper gives specific details of the courses offered. These include titles and brief descriptions, as well as a complete student essay.1
How can medicine discern when a fundamental change in its values is required? This was one of the far-reaching questions asked by an international group of experts for their report on the goals of medicine.2 Although many aspects of medical education remain relatively constant, the goals on the interpersonal side tend to shift as every new generation gives a different answer to the question: what do we want of our doctors? For a time, diagnostic and technical skills seemed paramount. But many of today's patients claim that a third skill is equally important. Benjamin described how, for thousands of years, the doctor's basic toolkit consisted of “the herb, the knife and the word”.3 Yet somehow this last has not been pursued with the same vigour as the other two.4 Doctors need humanistic skills. Perhaps more than at any time in the past, we need doctors who are able to respond sensitively and helpfully to their patients' emotional needs.
Although there is a large range of treatments available to cure many of the most prevalent illnesses, there are still many conditions that are not amenable to fast, successful treatment. Furthermore, doctors whose patients have, for example, cancer, heart disease, arthritis, or mental disorders must increasingly offer treatments that in themselves cause suffering. For many patients the technological side of medicine can elicit dread. Anticipatory fear of side effects may mean that visits to the doctor are postponed or recommended treatments and drug regimes are not followed. The dramatic rise in the number of patients attending alternative practitioners suggests that many people may now prefer the consolation of kindness to the perceived physical and psychological harshness of modern medicine.5
Thus it could be argued there is an increased need for doctors to be able to understand and respond to a variety of emotions in their patients, and many have further argued that the study of medical humanities could be “a means of producing more empathic and effective doctors”.6 Before attempting to introduce a new discipline, it seemed appropriate to look at existing strategies. There was already a good communication skills course in the core curriculum. But knowing the techniques of good communication does not necessarily mean that a doctor will use them. This problem, in turn, was addressed in part by the introduction of medical ethics. The duties owed the patient include respect for autonomy, beneficence and non-maleficence, and these provide a clear rationale for the use of good communication skills in every doctor-patient interaction.
But even if young doctors know how to communicate understanding, and know they have a duty to do so, there is still the problem of knowing when and how to recognise what is needed. How can young students with little experience of life or suffering be expected to understand at a deep level, what their patients are going through? Paradoxically, at the very time when society is asking for doctors who have an increased understanding of patients' thoughts and feelings, we continue to attract students whose backgrounds have left them less, rather than more, able than many of their contemporaries to cope with these requirements. This is not the fault of the students or the selection processes. Medicine still needs exceptionally good minds to cope with the extent and depth of knowledge essential for safe practice. It does mean, however, that curricula need to be reshaped to take account of the new requirements.
SQUEEZING CURRICULUM TIME
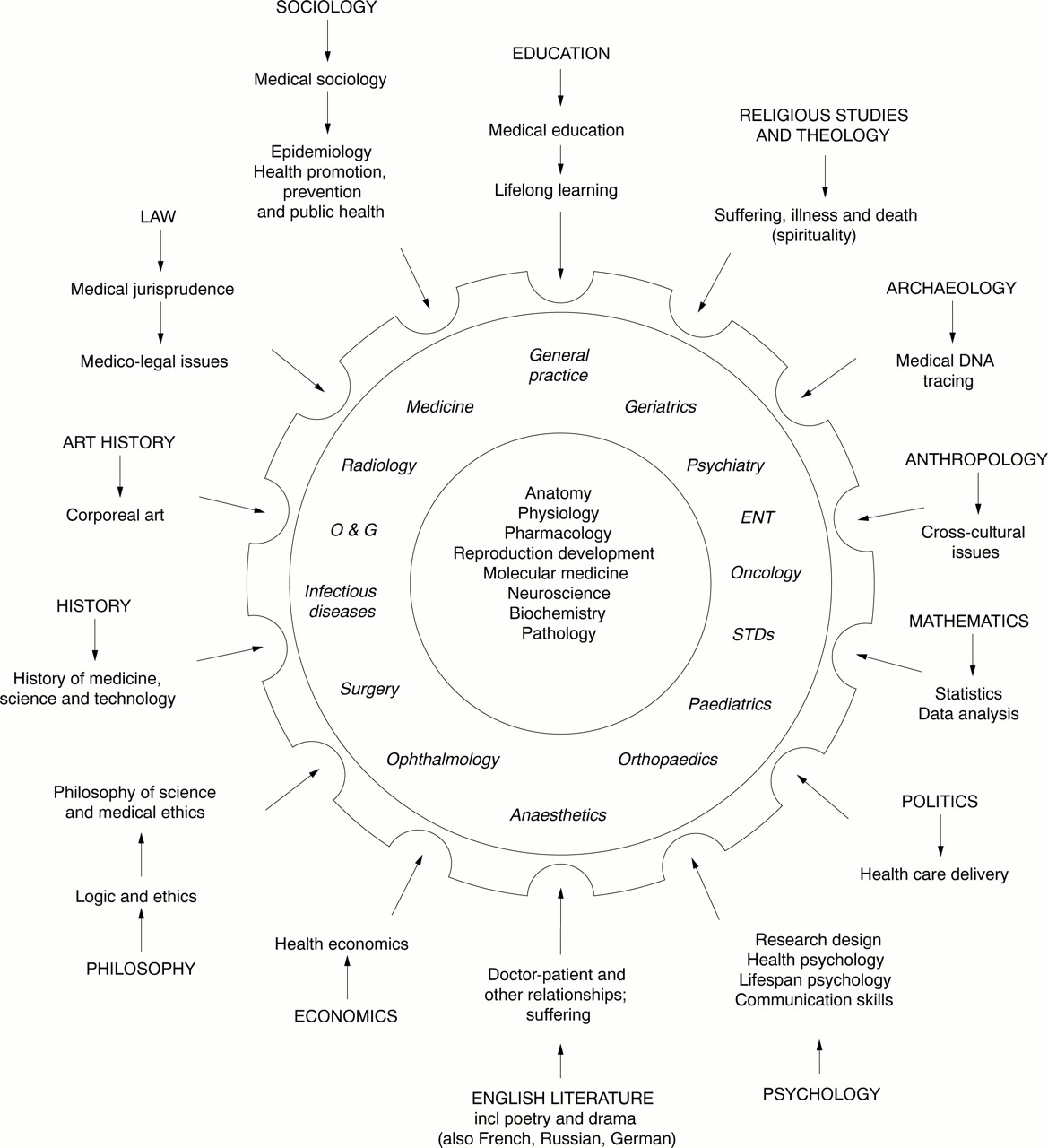
Competitive pressure on the curriculum has been described as the norm for as long as there has been a discipline of medical education, but it does seem to have intensified during the last decade. During that time, if not earlier, almost every major discipline in arts, law and social sciences has developed a branch that contains an interface with medicine, many of these achieving strong acceptance within their base disciplines.
The rise of these subspecialties has had a mixed reception from medicine. As noted above, some, such as philosophical medical ethics and psychology's communication skills, have been accepted by many educators and incorporated into the medical curriculum. Others, such as health economics and medical anthropology, have been regarded as peripheral. Some educators have welcomed these disciplines' broadening perspectives; others have regarded their proponents as “academics who congregate like vultures at the margins of medicine” merely to reinforce their own professional status.6 Supporters of the new initiatives in medical humanities argue that medicine is the better for being aware of, and knowing something about, these new subdisciplines.
In many schools, controversies have been settled and curriculum pressures partially solved by introducing options or special study modules (SSMs), a tacit acknowledgement that while these subjects may be of interest and relevance to doctors, they are not core. To introduce new elements into the core curriculum, a stronger case must be made.
REASONS TO INCLUDE HUMANITIES IN THE CORE CURRICULUM
1. To increase understanding of the human condition
As mentioned above, the first, and to most people the most obvious, part of the rationale for the introduction of medical humanities is that studying the human condition from the perspective of one of the arts or social sciences, may lead students to a fuller understanding of their suffering patients. Furthermore, in the future this fuller understanding of patients may, in turn, lead to a better understanding of illness itself, offering better insights into its nature, causes and outcomes. That is, instead of being merely additive, study of the humanities may be integrated into medicine by means of new and as yet little understood pathways.7
For many years, the primary requirement of core medical training could be summed up by referring to the development and production of a safe doctor. But today, many would argue that the phrase “safe doctor” should include the ability to interact with patients in a perceptive manner. Patients do not feel safe, and may not even be safe if doctors either fail to communicate, or do so in such an insensitive way that their advice goes unheeded. Failures in communication and understanding are said to contribute a disproportionate amount of the difficulty in cases coming before medical disciplinary committees. A minimum amount of training in at least some aspects of medical humanities may lessen the likelihood of this happening, as students learn the critical value of the doctor's verbal and non-verbal responses to their patients.
2. To expose students to the critical analysis of ideas
A second, and to some more persuasive reason for studying the humanities has to do with the nature of medical education. Of necessity, technical competence in medicine requires the acquisition of a series of specialist vocabularies—the languages of biochemistry, genetics and pharmacology as well as the traditional languages of anatomy, physiology, and the clinical disorders. This in turn means that much of the student's time must be given to memorising. Yet such is the continuing popularity of medicine that it attracts some of the most able students in every generation. In evaluating the curriculum, many educators point regretfully to the absence of opportunity to expose this particular group of students to higher order cognitive challenges, especially those involved in the critical analysis of ideas as exemplified in such disciplines as philosophy, classics and law.
3. To make more allowance for individual differences
It could also be argued that where students have had the benefit of a short compulsory course in one of the medical humanities early in their training, they are better equipped to select an individual pathway consonant with their individual interests and long term career goals. Many students, having done the compulsory component may decide these disciplines are not for them. Having derived the known benefits of study in these areas, they are then free to choose further options with a clear medical or research base. Others, however, having discovered an interest in one of the humanities, can be given the opportunity to continue study in their chosen field.
Thus the introduction of medical humanities as a core part of the curriculum may help to moderate the “conveyor belt” aspect of medical education, an advantage already experienced by schools running successful options programmes.
When this happens there is a double benefit because it not only provides for individual differences among students but also allows them to think more carefully about the variety of careers which can arise from the basic training. Medical graduates go off in a wide range of directions, from ophthalmic surgeon to psychiatrist, from endoscopist or radiologist to general practitioner specialising in family problems. These specialties require different temperaments as well as different skills. Thus it could be argued that courses that take account of, and allow for, the development of differences in temperament might contribute more to the overall needs of the discipline of medicine. Since competitive entry into medical school still means students are in the main obliged to follow uniquely scientific pathways, many have to defer interests in the humanities. Where the study of humanities is not introduced, at any level, doctors can graduate from medicine ignorant of the very existence of the humanities' contributions to their discipline. It could be argued that such graduates are educationally deprived, since they don't know what they don't know.
4. To provide pockets of expertise and lifelong interests
Where students have been given a choice of discipline within medical humanities (such as in the system described below) there have developed small groups of students in every cohort, with specific, extra knowledge. These have come to provide “pockets of expertise” for their fellow students. It means that within every class of medical students, a few will become known among their peers as the ones with some, albeit limited, knowledge of how, for example, the legal or political systems work. Students who have begun their studies as undergraduates in these areas may find in them the basis for lifelong interests. Some will have expertise in medical sociology, medical archaeology or anthropology, some will have been introduced to medical issues in art, literature, history, or theology. Students who become known for their particular interests or skills may be able to offer informed opinions when their future colleagues are thinking about related problems.
It is also our hope that, at the individual level these interests might stand students in good stead in the future. They may help by providing an alternative perspective (anthropology, sociology, history), a breadth of interest (art, literature) or involvement (law, politics, theology) which could help in coping with the rigours of professional life.
THE ROUTE TO ESTABLISHING A NEW COURSE
A series of committees over the years tackled what became known as “the whole person” problem. This appeared to have a double application. The first referred to treating the patient as a whole person, which included the duty to respect patient autonomy as well as the duty to learn and use good communication skills, and sought to advance a more compassionate understanding of the patient's situation through the study of the humanities. The second application was to the doctor, who as “a whole person” him or herself would not only be enabled to better understand the patient's problems and suffering, but be better able to cope with them, sustaining less personal stress and having more personal resources for coping with the inevitable pressures, crises, and tragedies which all medical practitioners encounter in the course of their duties.
Earlier committees were less than successful, having drawn all they could from psychology and sociology. A later, interfaculty committee, consisting of representatives from arts disciplines as well as medical specialists, fared better. Lengthy, often spirited debates resulted in agreement on two principles which would underlie all decision making in the introduction of the humanities into the medical curriculum.
The first non-negotiable requirement was that courses would be taught only by people accredited and approved by the discipline. No matter how enthusiastic the would-be lecturer, he or she would not be invited to teach unless the head of the corresponding department in the arts or law faculties approved the appointment. This was the primary requirement of the arts faculty committee members. For the medical committee members, the primary requirement was that each course should be clearly relevant to medicine. No matter how fascinating or topical the current issues within the discipline, the course had to be such that studying the material would result in improved patient care.
Papers were designed and trialed as option papers for the first five years. This gave the opportunity to refine course content, respond to suggestions (both lecturers' and students') and solve assessment problems. Then, for the first time, in 2000, the medical humanities elective became compulsory. Eight courses were offered from which all second-year students, no matter what their background, were required to select one. The courses were from the disciplines of law, philosophy, sociology, political studies, classics, English literature, history, and art history. Students were asked to give first, second, and third choices, but such was the spread of students' interests that almost everyone got their first choice. Average class size was fourteen, and none was larger than eighteen.
Teachers were enlisted from a variety of sources, but as agreed, all were ratified by their base disciplines in the other faculties. Some were recent PhD graduates; others were recently retired. Each consulted individually with the medical humanities coordinator about the design of an appropriate paper. In line with the overall goals of the course, the critical analysis of ideas was to be given a central role. Small group sizes ensured that all students could be given the opportunity for discussion and debate. In fulfilment of the requirement that all papers should be seen to be relevant to improved patient care, particular attention was paid to content. None of the disciplines had any difficulty in selecting such material.
ASSESSMENT AND EVALUATION
Policies and strategies regarding both student assessment and staff evaluation were agreed on at meetings held before the courses began. Policy decisions on assessment were made by the group. Most teachers decided to give about 30% of the marks to a seminar presentation and 60% to a final review or research essay. It was considered undignified to give a mark for attendance, but since debate and discussion were key elements of the course, most teachers gave 10% to “contribution to class discussion”.
It was thought there might have been difficulties attaining intergroup consistency in assessment. All final essays and teachers' mark sheets were handed in to the coordinator so that distributions could be checked. Teachers were assured they would each have the final say in rank ordering. Even so, some of them said they would be very reluctant to have someone else adjust or realign their overall mark distribution for any reason. Others feared that if students thought it was easier to gain high marks in a particular discipline, enrolments in subsequent years might be distorted.
As it happened, marks and distributions were remarkably consistent. Teachers were pleased with the responsiveness, intelligence and originality of the students and were happy to accept a recommendation that so far as possible, marks conform approximately to a normal distribution curve. Final marks were consistent across all groups.
Towards the end of the semester, all the courses were independently evaluated by staff from the Centre for Professional Development (CPD). Most items were selected from a standard item bank. In addition there were some new items, designed to find out what students thought of the introduction of a compulsory medical humanities course into the second year of medical training. Teachers approved all items in advance.
The student response rate was 91% (106 evaluations out of a possible 116 students enrolled in the course). Raw data were given in a five-column grid, reflecting responses to questions (strongly disagree, disagree, neutral or don't know, agree, strongly agree). Data were manipulated by CPD staff to give a mark out of ten.
On the standard items, ratings for the medical humanities teachers were either comparable to ratings from university staff as a whole, or better. For example, the mean rating for humanities teachers on the item “Lecturer responded to students' questions in a constructive way” was 8.07 compared with the university-wide figure of 7.35. All humanities teachers rated higher than the average for all university teachers on the item “Lecturer showed enthusiasm for the subject”, with five teachers gaining scores above 9.00 compared with the university-wide average of 7.88. These high scores were informally ratified by several instances of unsolicited student comment and particularly applied to the two papers which gained the highest aggregate ratings from students, Politics of health care delivery and Medicine in literature. The overall high scores in this area may, however, be in part an artifact of the newness of the courses, reflecting the “optimism and promise” remarked on by Meakin and Kirklin.8
In addition to teacher ratings, students were asked their opinions on whether medical humanities should be included in the curriculum at all. Responses to these items showed wider variation than the teacher ratings. For example, average responses to the item: “The course opened up new areas of interest for me” fell between 5.56 and 8.46 with a mean of 6.88. Unfortunately, as students later pointed out, this item was not well designed. Some students who had enjoyed English literature at school may have responded “disagree” or even “strongly disagree” on the grounds that the course was not a “new” interest.
The item: “The medical humanities courses are an interesting addition to the medical curriculum” received a mean score of 7.00 with a range from 5.47 to 8.46. Since it was well known that some science-oriented students (and faculty members) were not in sympathy with the new initiative, a bi-modal distribution on these items was expected.
FOLLOW UP
In the third year of their undergraduate degree students have the opportunity to take one more options paper. Some students chose to further their studies in the humanities by taking a related or more advanced paper in arts, law or social sciences. Other students chose medical research options or other specialist medical papers.
It is not known whether these new initiatives will be continued in the future. Much will depend on the commitment of staff and senior faculty members, which in turn depends on whether they remain convinced of the academic and professional value of the papers. On the larger stage, such initiatives need to be accepted and ratified by community groups who in their turn represent the wider society. Like all curriculum changes, courses in medical humanities will need to be constantly reassessed and re-evaluated to ensure they continue to contribute to the training of the kinds of doctors contemporary society needs.
{kind=link}
Pressures on the medical curriculum. Core sciences are central to clinical sciences. Other disciplines have contributions to make