Article Text

Abstract
The existing literature on leadership often describes it within fairly rigid gender roles. Entire models of leadership have been ascribed gendered labels. Shared leadership is, in traditional leadership theory, a feminine model. After observing a National Health Service (NHS) department enacting a shared leadership model, and using ethnography, grounded theory and comics-based research, we decided to explore the relationship between shared leadership and gender stereotypes. We realised our hope was to see a subversion of traditional stereotypes. Our data showed shared leadership overall as a feminine model, with its focus on distribution and compassion. Within the group, a range of gender roles were performed, meaning that the group could represent itself to the outside world as either more masculine or more feminine as required. This was beneficial, as conflict with outsiders was minimised and hence anxiety reduced. However, we noted that within the group, traditional gender roles were not subverted and were probably reinforced. Despite our view that shared leadership has not been an opportunity to resist gender stereotyping within this department, the success of this feminine model may represent a challenge to the prevailing masculine model of leadership within the NHS.
- comics and medicine
- gender studies
- graphic medicine
- social anthropology
Statistics from Altmetric.com
Introduction
Historically, public discourse has focused on leaders as heroes. The shifting landscape of the National Health Service (NHS) has led many to believe that we need to move beyond the antiquated model of heroic leadership.1 This classical stance is slowly giving way to ‘postheroic’ models of leadership which value leadership as a malleable process that is shared and distributed.1–4
Leadership attributes have become gendered through binary, social constructions—the masculine and the feminine. Similarly, entire models of leadership have been prescribed gendered labels, with classical heroic leadership often being seen as masculine4 and models of leadership that emphasise collaboration, compassion and collective growth being seen as feminine.4 5 The development of these gendered attributes is closely linked to ideas pertaining to work and home. For example, domestic work is thought of as feminine and therefore lower status.6
In the NHS, men have often dominated leadership roles,7 particularly within medical and surgical departments as well as the overarching executive. Although women are increasingly taking up leadership roles, men continue to dominate these positions.8 Furthermore, heroic (masculine) forms of leadership have proven remarkably resilient, because of notions related to ego and the ‘romanticising’ of heroic leadership.5 9 10 There is therefore a weight of history and taboo, which dictate how leaders are expected to act in healthcare.
The department we studied in an acute teaching hospital in England currently enacts a flattened leadership model, which takes inspiration from the practices of shared leadership. We explored the department’s transition from a heroic to a postheroic leadership model. The strongest theme to emerge from our data was the presence of gendered leadership stereotypes.
In this article, we will introduce the key theoretical standpoints, give a background to the case study and comment on our findings and their implications. In the next section, we will discuss the concepts of shared leadership, gendered leadership and performative acts of gender and leadership.
Shared leadership
Postheroic models of leadership such as shared leadership (also known as collective leadership) emphasise the role of multiple actors, who actively take up leadership roles formally and informally.1 Leadership moves away from the attributes which identify it as a noun and metamorphoses to become an active process, a verb.11
Shared leadership is seen as highly practical in the healthcare setting12 13 as the nature of delivering healthcare requires much collaboration.14 The benefits of shared leadership impact on four perspectives: individual, coworker, organisational and societal.4 These result in benefits which include the avoidance of hubris, greater representation and a greater sense of security.4 15 Conversely, critics of shared leadership have noted that resistance to the model can make implementation extremely difficult. O’Toole et al stated that ‘in the popular mind, leadership is always singular.’ (O’Toole, p. 64).16
Gendered leadership
We believe gender plays an important role in leadership behaviour. Eagly and Johannesen -Schmidt6 argue that agentic and communal aspects of gender roles are particularly pertinent. Agentic attributes—competitive, dominant, self-confident—are deemed to be masculine, while communal characteristics—nurturing and interpersonal sensitivity—are deemed to be feminine. Regardless of organisation role, studies in the workplace have shown women to behave more communally than men.17
Agentic traits, such as individualism, control and assertiveness, are socially ascribed as masculine and are seen as traits of heroic leadership.4 6 Particularly in the realm of hospital leadership, the lens of history must be assigned to heroic leadership as men have often dominated leadership roles and thus masculine attributes have been perceived as the ‘norm’. On the other hand, postheroic models, which place emphasis on inter-relational work, compassion and empathy, are seen as feminine.4 5 18
Performative acts: gender and leadership
In this section, we will uncover the construction and deconstruction of gender and the development of leadership through performance.
Andrew McMillan states, ‘leadership is a performance: so be conscious of your behaviour because everyone else will be’.19 Kotter’s definition of leadership is concerned with aligning, motivating and inspiring people.1 20 To be able to align, inspire and motivate, performance as a leader is ultimately decisive. Likewise, Yukl’s taxonomy of effective leadership describes leadership attributes which can be enacted as part of leadership performance.21
Gender, in the eyes of Judith Butler, is constructed through a series of performative acts.22 23 Her work serves as a key theoretical pivot for us that aligns leadership, gender and the construction of gendered leadership. This alignment is particularly important within a healthcare system where leadership is dominated by men and masculine attributes.
Butler argues that gender is devised through performance.22 For Butler, gender is ‘what is put on, invariably, under constraint, daily and incessantly, with anxiety and pleasure’ (Butler, p. 531).22 Yet because gender is constructed through the repetition of performative acts then she argues that there is a subversive space formed that would allow the development of a different gender. The performance of gender, however, is dictated through socially constructed, binary notions and the lens of history. Butler therefore argues that we are often discouraged from the subversive space because of social expectations and taboos. Gender is ‘constrained by available historical conventions’ (Butler, p. 521).22
Gendered leadership is a powerful combination of both performances that are defined by history and taboo. If heroic leadership is considered standard within the NHS, then conventions have constrained leaders to perform with masculine leadership attributes. Furthermore, as women take up more leadership roles, there is an emerging conflict. Enacting a congruent gendered leadership performance—that is, a woman performing feminine leadership—is often considered mundane and may potentially be demeaned as doing what women do.5 On the other hand, women whose leadership performance follows the path of history (but contradicts her socially perceived gender) are often met with negativity and resistance,24 thus making the subversion of gendered stereotypes difficult.
Alongside specific leadership behaviours, we also consider speech and body language as examples of performative acts. These play a crucial role in the construction of gender and leadership. The work of Tannen also aids our understanding of the group through the way they talk.25 Table 1 summarises the characteristics of gendered talk that are pertinent to our study.
Summary of contrasts between masculine and feminine talk as expressed by Tannen25
Case study
Although much of the literature discusses organisational commitment to shared leadership (West et al, 2011),26 the department we studied have undertaken the practice of shared leadership in a clinical microcosm. In this context, the leadership group consisted of seven consultants across two sites. The whole department are responsible for approximately 150 inpatient beds, community services and clinics. Although other consultants, nurses, allied health professionals and junior doctors were involved with the leadership group, none were permanent members.
In 2015, the department was experiencing a tumultuous period. Due to the anxieties and pressures placed on the clinical lead, the position became untenable. The department therefore moved to a shared leadership model, where all the consultants took on leadership responsibilities to spread the burden of anxiety within the department.
In such stressful times, there might be a desire to engage in strong, heroic leadership in order to provide safe care to patients. It was stressed however by the consultant body that a such multi-faceted department carries an almost unmanageable and off-putting burden of expectation for a solitary, heroic leader. To combat this, a thoughtful reimagining of the role of lead occurred within the department in April 2016 and the clinicians decided to embrace a shared leadership model.
The model used stresses a flattened structure where all consultants have leadership responsibilities regardless of previous experience. Roles (such as governance, junior doctor staffing and acute floor) were distributed among consultants and a weekly Monday meeting with an agenda was instituted. While there was no prescribed ‘leader’, there was a face for the change, in the form of the Monday meeting chairperson. The chairperson also received the email traffic and constructed the weekly agenda. We felt that the meeting was a space where decisions were made and tasks distributed. The meeting, as an anthropomorphised entity, was arguably the leader.
Methodology
Research conducted in the healthcare setting often relies heavily on quantitative measures.27 We have decided on the use of qualitative research methods, in particular ethnography, as they allow for the analytical exploration of the psychosocial aspects of leadership practice.
Leung defines ethnography as a ‘social research method occurring in the natural setting characterised by learning the culture of the group under study and experiencing their way of life before attempting to derive explanations of their attitudes or behaviour’ (Goodson, p. 2).27 Although mortality, morbidity and length of stay data can be analysed to discuss the impact of clinical leadership on patient safety, we believe that quantitative methods would not capture the complex sociological and leadership motifs experienced in any transition from heroic to postheroic models of leadership. Ethnography, on the other hand, has allowed us to explore the culture within the group and derive an explanation for the complex leadership behaviours and attitudes on display.
Alongside ethnography, we have also used a comics-based methodology.28 Comics are a relatively new addition to visual methods within arts-based and practice-based research. They offer a way to explore the complexity of ethnographic data, as they can represent multiple layers within a narrative structure. This is achieved through drawing style, speech and thought bubbles, visual symbols (such as a light bulb for an idea) and the use of the gutter to allow the reader to make connections between the panels. Close reading of comics also gives access to unconscious and emotional responses to events, which allows the research to become more reflexive. The use of humour and satire within comics means they can be subversive. This feature fits with our desire to resist established masculine leadership practices while also challenging traditional academic discourse.
Methods
Raw, ethnographic data were collected in the form of field notes primarily from observations of the weekly meeting of the consultant group. One of us observed the group silently throughout the meetings, while the other acted as chairperson. One author had previously worked in the department as a foundation doctor and so was aware of some aspects of the consultants' personalities but had no prior knowledge of the workings of the group. The other author had been a consultant in the department for more than 5 years and was fully integrated into the group. We therefore had etic and emic perspectives to the leadership group and collection of data. Raw data were also garnered from a variety of interactions between ourselves and the consultants. Both researchers kept research journals to record the contents of informal interactions and discussions related to shared leadership, as well as their emotional responses when appropriate.
Data collection began in April 2016 with regular attendance by the observer. Frequency of attendance by the observer was reduced in August 2016, as we felt the data had reached saturation. Due to the logistical demands of the Foundation Programme, the observer was unable to attend between January and March 2017. This allowed for a fresh perspective of the leadership group on the observer’s return. In total, 10 meetings were observed, coded and analysed.
Alongside the observational data, we conducted three free-association narrative interviews29 with members of the group (M1, F2 and M3 according to table 2). The consultants were selected via purposive sampling due to their differences in leadership experience and length of time within the group. One manager was approached for interview; however, no response to our invitation was gained. Interviews were recorded on a mobile device and then manually transcribed.
The core participants within the shared leadership case study
Our research question was developed using methods based in grounded theory. One author coded field notes and interview transcripts manually, examined for recurring motifs and then wrote analyses using a series of theoretical lenses. Following discussion and reflection of these analyses, the other author produced comics in draft form, which were then sent to the first author and discussed again. The first author then wrote further analyses of the comics. This iterative process was our way of triangulating data, ensuring reflexivity and sharing our knowledge of pertinent theoretical views. Through this process, we eventually agreed to focus on gendered leadership as the most surprising and interesting area of our research. We also used comics to seek the views of our participants on shared leadership; they drew comics and explained them to us. The second author later amalgamated these into one comic. Some of the comics produced are used in this paper to illustrate our findings.
Ethical considerations
The study was deemed not to need any formal ethical approval by our Trust research committee. It is important however to discuss some of the key ethical considerations linked to the study. The study was explained and written consent was obtained from all participants prior to the observed sessions and interviews.
We were mindful that one researcher is a member of the leadership team, while the other researcher has previously worked with members of the consultant body. This created possible areas of tension with colleagues which we minimised by checking with each other and the participants whether our analysis was fair and likely to offend others. All comics and this manuscript were shown to all participants prior to submission, for feedback. We tried to balance the need to tell the story as we saw it, with regard for the potential emotional impact on our participants. While it is impossible to settle on one ‘true’ version of events, we wanted to make sure that the story we told was representative enough of the participants' recollection of what happened. For example, one participant asked for the wording of one comic to be altered slightly, and this was clearly very important to them and the way they were portrayed. We felt it did not significantly change the story or meaning of the comic, so agreed to alter it.
Results
In this section, we present our data analysis. We have used a selection of comics to tell the story of our observations around the themes of: the persistence of heroic, masculine leadership and gender roles; the right man or woman for the job; shared leadership as a feminine leadership model and the struggle to subvert gender stereotypes. Each comic is then analysed through the lenses of leadership and gender supplemented by further examples from observations and interviews.
In order to provide context to the narrative of the case study, table 2 presents a background to the core participants involved within the study. Their anonymised labels will be used throughout the presentation of the results. For convenience, we have labelled participants using the binaries of male and female, as they presented to us.
The persistence of heroic, masculine leadership and gender roles
In 2015, the department was experiencing a tumultuous, transitional period. New clinical directorate leads (M1 and M2) were appointed. The traditional perspective of leaders as heroes instantaneously prevailed and with that connotations regarding masculine leadership.
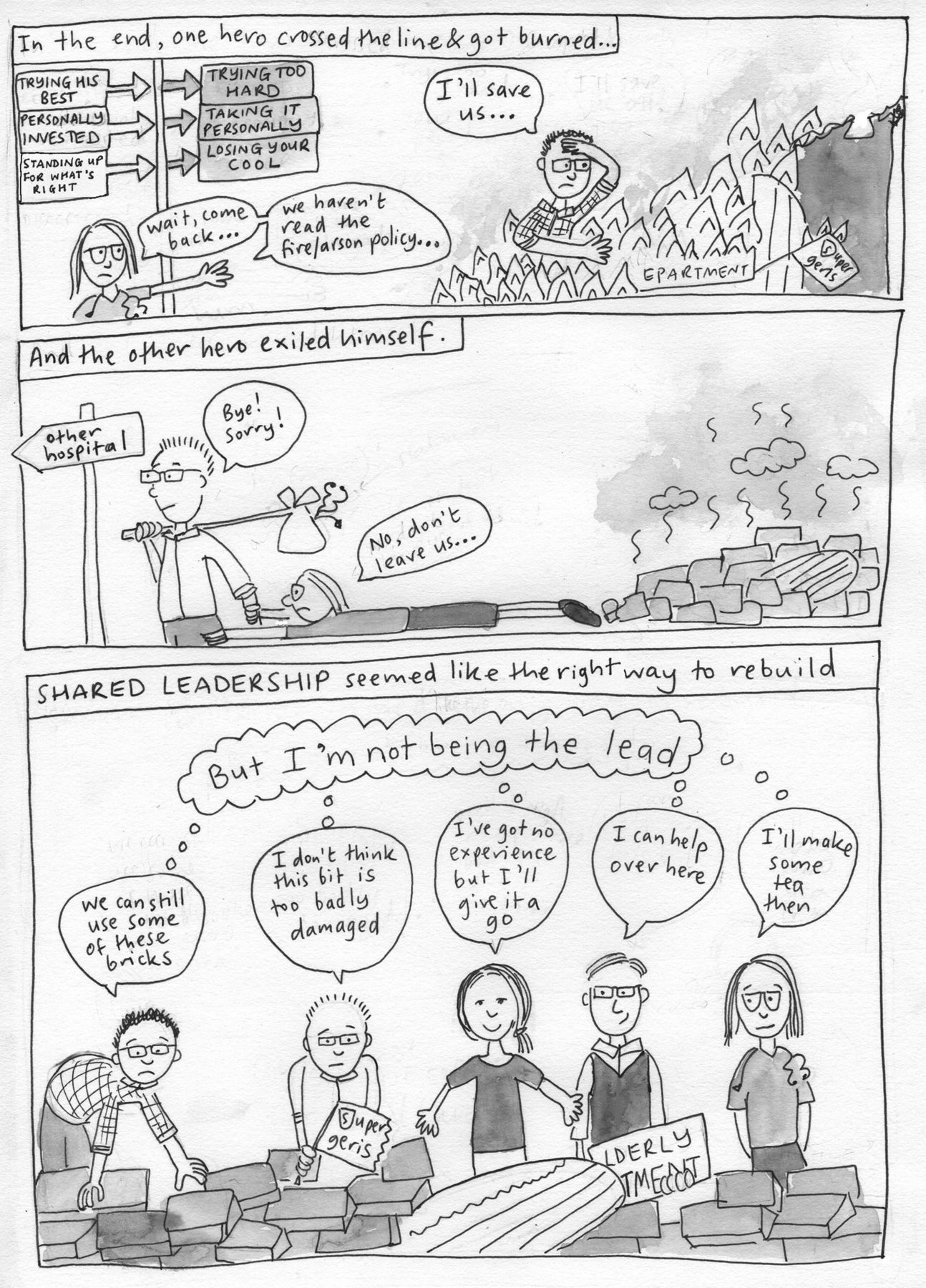
The comic (shown in figures 1 and 2) presents on its surface of men performing heroic, masculine leadership. The comfort provided from this congruent display of gendered leadership is one that links to clinical leadership within the NHS—men have often dominated medical leadership roles, therefore masculine leadership and its attributes are seen as the apparent norm.
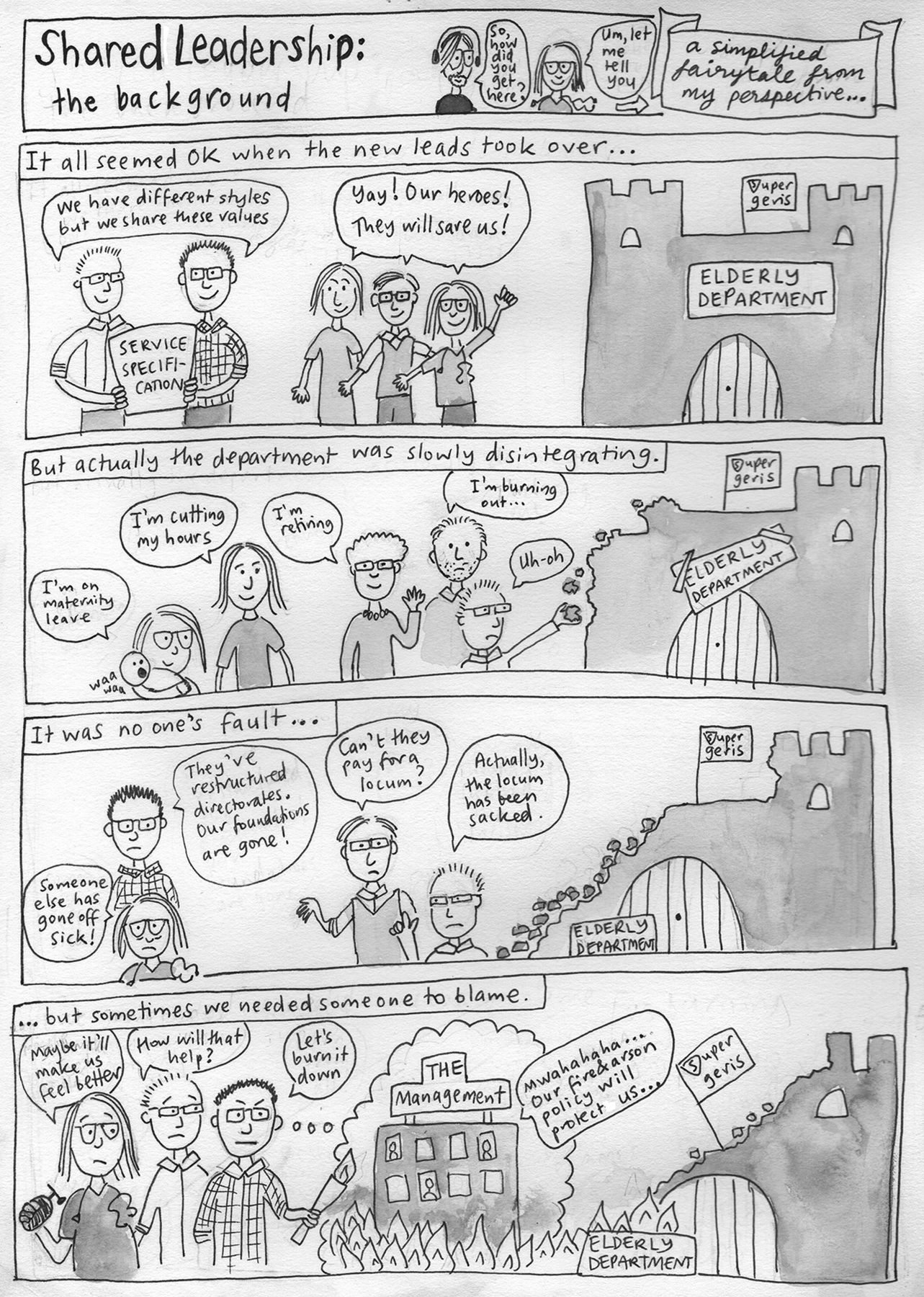
Shared leadership: the background (part 1).
Shared leadership: the background (part 2).
Heroic leadership, and thus masculine leadership, is often championed within times of anxiety and uncertainty.5 8 As shown, clinicians were leaving for a plethora of reasons and heroic leadership was seen as the presumed answer. Interestingly, we noticed the depiction of the mother (F1) within the comic, which will be alluded to further but underlines one of the many gendered forces at play within the realms of work and hospital leadership.
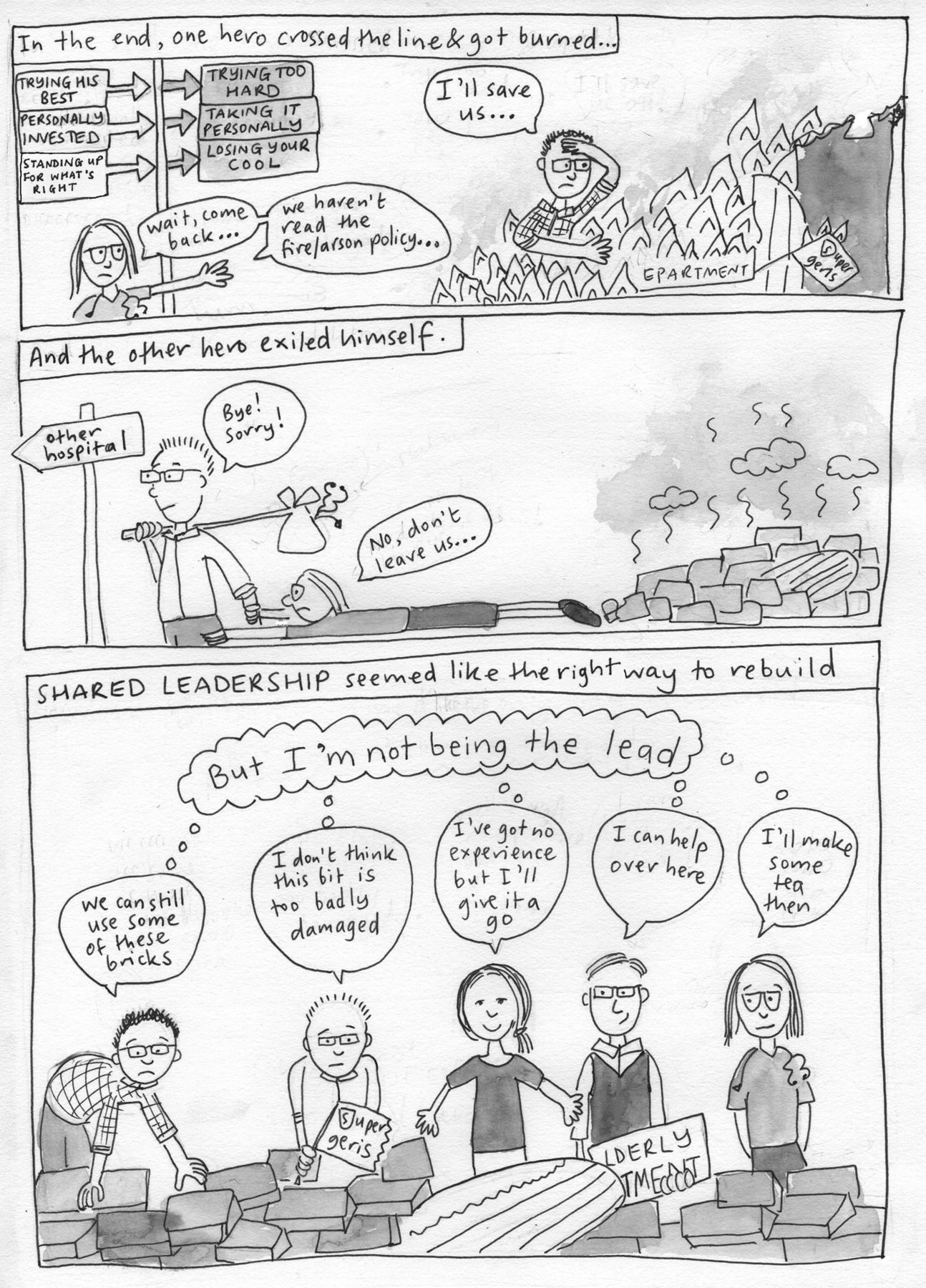
The key image presented within the comic is that of our male leader (M1), enacting heroic, masculine leadership and walking into the metaphorical fire (see the first panel of figure 2). There is the implication presented that in order for M1 to perform masculine forms of leadership, he is expected to walk into the fire and he must continue to be the hero. His gendered leadership behaviours are therefore somewhat socially constrained.
The gender roles, which are presented within the background comic, have been remarkably persistent throughout a year’s worth of observation. M1, regardless of historical events, remains fixed within masculine attributes of leadership. M1 described himself as, ‘a blunt man’, an ‘innovator’ and is perpetually concerned with recognition for the work he is doing as a doctor. M1 is the only member of the group to use an electronic banner displaying the group’s award in service innovation. M1’s speech was littered with conflict and status talk.25 There was a constant focus on clinical performance, be it his own: ‘I could not maintain performance’ or the department’s ‘intense review of metrics’. For M1, the end result was always deemed the most important matter even when discussing interpersonal matters. For example, during a dialogue regarding the sensitive concerns of a colleague, M1’s response was, ‘what is the endgame here?…because you won’t get what you want from X’.
It is, however, not just M1 who we see persist with a gendered leadership identity. As shown through the mother and child within the comic (figure 1), F1 has also seen herself shackled to constructs closely linked to feminine leadership. Even though the model preaches a flattened structure, the chairperson of the Monday meeting (F1) was the primary spokesperson for the model. Using shared leadership—a feminine leadership model—to bring about change has seen F1 placed clearly within the role of the ‘mother’. At times, F1 spoke candidly regarding her parental role within the group and was even referred to as ‘Mum’ by members of the group in a jovial conversation.
Her feminine leadership performance has included explicit acts of nurturing, kindness and selflessness: ‘this is where your voice is important’, ‘our unity is our strength’ and ‘the trouble will come to me [acknowledging the damage of angry emails by colleagues]’. This is at odds with F1’s expressed gender role outside of clinical leadership. Enacting a feminine leadership performance, while congruent to her perceived gender is at odds to her own gendered view, ‘I am very much the Dad at home’.
The shared leadership model therefore sees the persistence of set gender roles. M1, the previous heroic leader, has remained unchanged. F1 performs a style of gendered leadership that is congruent to her outwardly perceived gender but incongruent to herself. As Butler22 23 posits, F1’s identity as a leader is created and performed by herself but also defined by the constructs surrounding her.
The right man or woman for the job
Figure 3 provides an interesting dichotomy within the practice of shared leadership and its relationship to gender roles.

Convincing the powers-that-be to allow a revolution.
Particularly in the clinical directorate structure of the hospital, the practice of shared leadership is unique and peculiar. M3 expressed surprise when told the group was embarking on a shared model. He also highlighted his previous negative experience of shared leadership in an interview. He confided that while shared leadership seemed beneficial on paper, it was often difficult to maintain in small clinical groups due to a lack of commitment. M3 stated that it was not long before his previous group reverted back to heroic leadership.
Despite some reservations, there was a palpable belief within the group that shared leadership was potentially innovative within our Trust and a way to resist the pressures from higher management.
Although the belief was that their actions were ‘revolutionary’, the group’s use of gender roles remained in line with expected stereotypes. Although from the outside, there are a plethora of gendered leadership behaviours at play, it appears that individually the group quickly settled and remained in their own comfortable gendered leadership performances. The shared leadership model cemented and compounded this, as the distribution of the tasks meant that the right gendered leadership performance—masculine or feminine—was applied to the right situation. Members of the group were therefore never challenged to subvert gendered leadership stereotypes but in fact revelled in them.
The masculine, heroic leader (M1) of figures 1 and 2 could not have been sent to this meeting. The gendered leadership performance needed was one of friendly submission and supplication. As Fletcher5 would predict, F1 performed as a submissive leader, supplicating to her male manager, regardless of her inherent beliefs (the subtitles within the comic). This feminine performance, linked to archaic notions of masculine versus feminine power dynamics, has also been a source of internal struggle for F1 as rather than subverting gender stereotypes she has reinforced them.
Although the model has constrained F1 to perform as a feminine leader, it also allowed members to comfortably continue their performance as gendered leaders. M1 the heroic and masculine leader is used for governance, with its need for attention to performance and metrics. F2 who said ‘I never saw myself as a leader’ and expressed the view that female leaders concern themselves with understanding their colleagues, was charged with mentoring the junior doctors. Her performance as a leader, which contained rapport speech, proposals and questions is inherently feminine.25 She even acknowledges that she is not the right gender for the job: ‘I’m not the girl for finances’.
Finally M5, feminine in leadership style, who often brought matters relating to colleague welfare to meetings, was tasked as deputy-chair of the Monday meeting on several occasions. F2 suggested he was a ‘good replacement’ because of his ability to nurture the group.
The idea of women being submissive and supportive within the model has also been seen through the observation period. Supportive and proposal talk (from F1 and F2 in particular) highlight that even though there is a flattened structure, gendered power dynamics remain.25 F1, as chair, would bookend discussions to the group with ‘is that ok?’, and likewise begin sentences to colleagues with ‘do you mind?’. This is in stark contrast to the forceful language used by some of the male members of the group. Furthermore, F2 within her interview often asked, ‘what do you think?’ and sought reassurance, ‘is that right?…is that what you want?’.
Shared leadership as a feminine leadership model
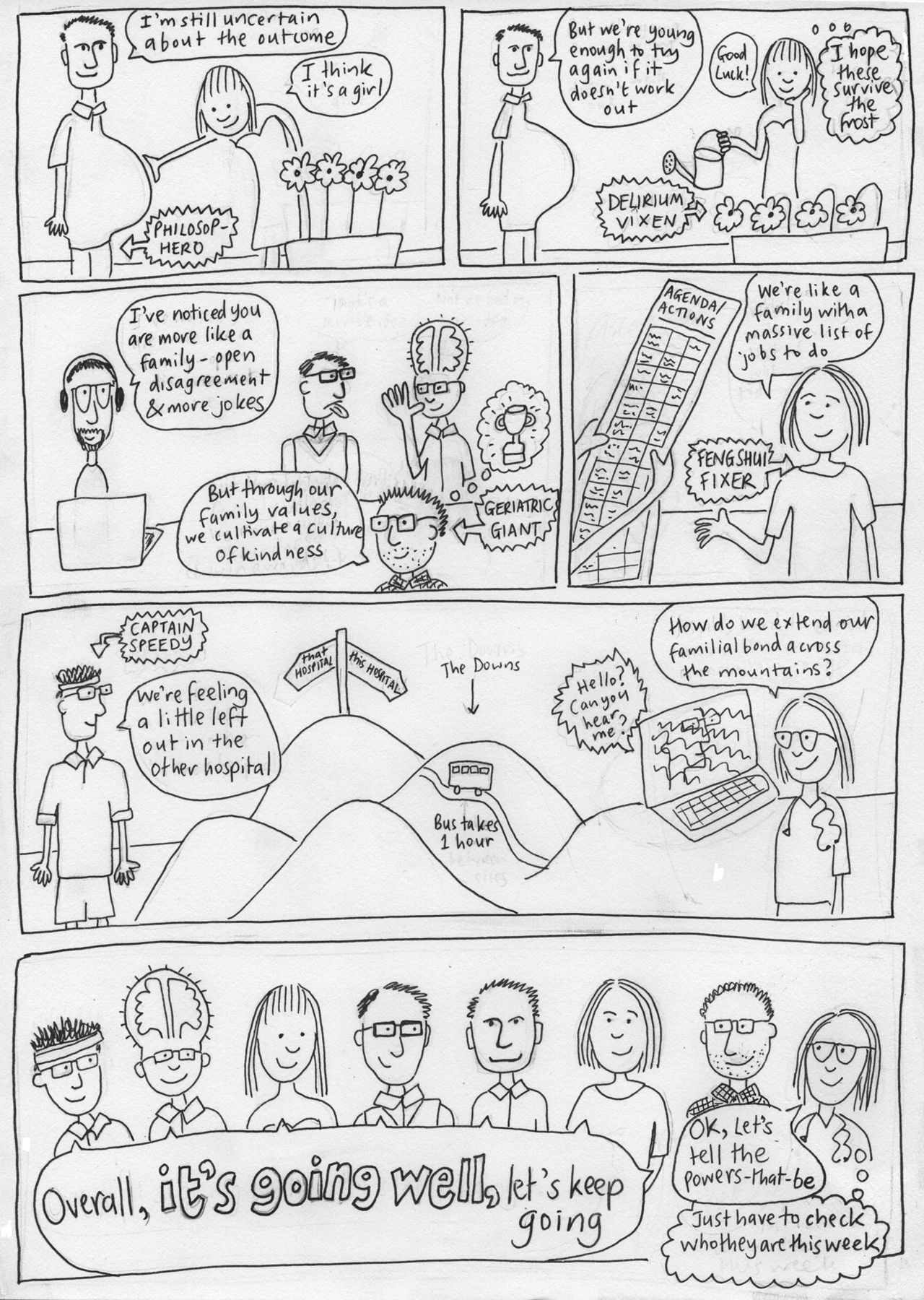
The origins of figures 4 and 5 are rooted in our chosen technique of validation: asking the participants to draw how they felt shared leadership was progressing after 6 months. We amalgamated these drawings into this evaluation comic.
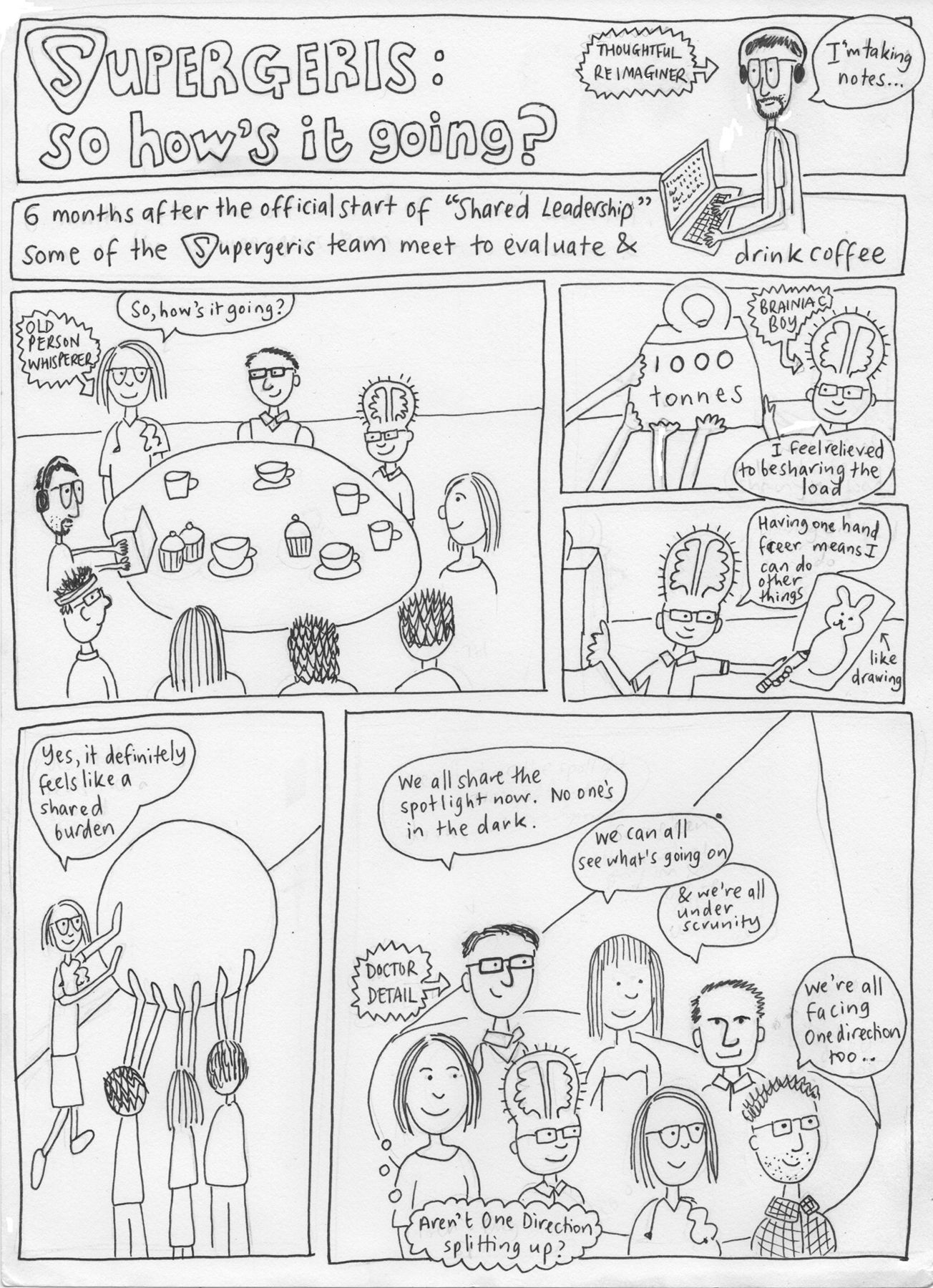
Supergeris: so how’s it going?—Evaluation comic (part 1).
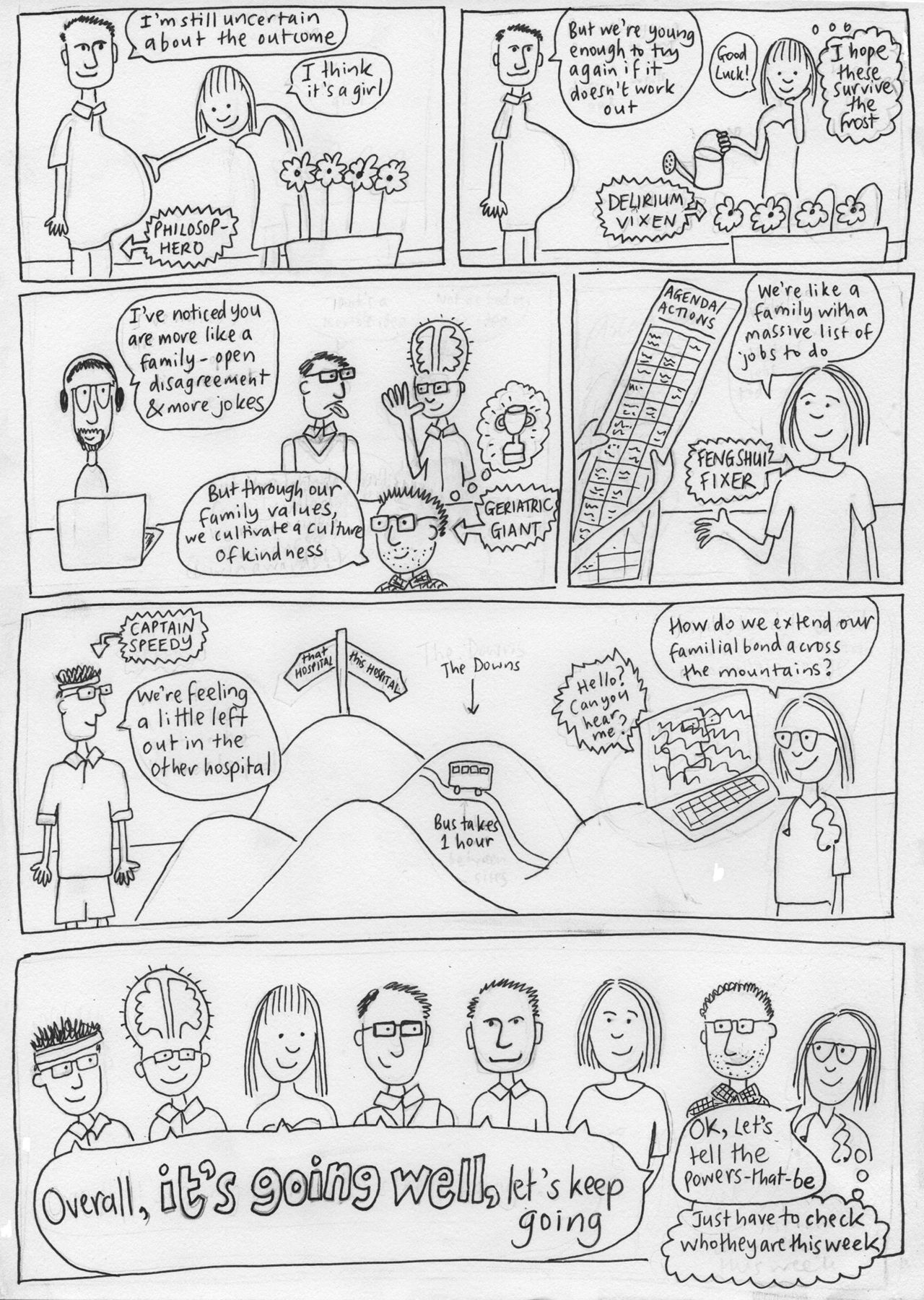
Supergeris: so how’s it going?—Evaluation comic (part 2).
Figures 4 and 5 depict a perceived reduction in anxiety and a convivial spirit within the group. There is the sharing of anxieties and work-based pressures as depicted through the 1000 tonnes weight, sharing of a spotlight and rolling the boulder against the steep, perilous landscape of delivering healthcare within the NHS.
This dissipation of anxiety was also noted in several of the interviews conducted. M1 clearly stated, ‘it feels a lot better’ and that with the development of shared leadership, there was now an ‘easier and more supportive forum’ for debate. This is in contrast to a heroic model, which ultimately left M1 ‘banging my head on a brick wall’. Likewise, F2 commented on how the model was a ‘really good way of distributing the burden and the stress’.
This development of kinship and kindness is what the group hoped to foster at the inception of the shared leadership model. With this in the mind, the group, 6 months on, was more familial. There were light-hearted jokes, at the expense of other members of the group, but also the presence of conflict. For M1, M3, F1 and F2, this was a positive indicator of how close the department had become. To all of them conflict indicated that no one was hiding.
What has been described fits notions of a shared leadership model that nurtures trust and loyalty from a group as they move above their own self-interest towards a common vision. As discussed within the introduction this style of leadership is commonly seen as feminine.4 5 It is therefore fitting that figure 3B’s opening panel shows a team-member predicting the outcome of shared leadership to be a girl. This comic was done prior to any work on gender commencing and helped us to realise our focus.
We feel the shared leadership model is democratic, nurturing, familial and distributed, all characteristics which would traditionally align themselves with feminine leadership.
The struggle to subvert gender stereotypes
Leadership, be it medical or otherwise, has had a frightfully taut relationship with binary constructs of gender. There is an almost definitive, black-and-white nature to some of the literature discussing gendered leadership. Our aim, once gender became our focus, was to explore gender stereotypes. We realised, through reflective discussion and analysis, that our hope had been to see a subversion of traditional stereotypes. This desire for resistance to the pervasive models of leadership in the NHS was perhaps one of the key unconscious reasons for adopting this approach to leadership and our research, although this only emerged through our exploration of the data.
As figure 6 shows, subversion is double-edged and dependent on the perspective from which one views the group. With the heady presence of compassionate, democratic leaders (ie, the feminine) mixed alongside laissez faire or heroic leaders (ie, the masculine), one could argue that the group is the best of both genders when viewed from the outside. If gendered leadership was to be seen as a spectrum rather than a binary, then our group (with its different members) moves fluidly along the spectrum.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The (doomed) idea of genderless shared leadership.
It was suggested by M3 within their interview that a good leader is one who is ‘flexible’ and knows when it is ‘time to be autocratic…and time for hand-holding within a technical bureaucracy’. The presence of multiple gendered leadership styles allows for a flexibility as the right performance can be provided. The plethora of gendered leadership behaviours found within the group fulfils theoretical traits of effective leadership as espoused by Yukl’s taxonomy.21
We feel that traditional feminine work plays a crucial role in a successful shared leadership model. It was suggested by M3 that in fact the group ‘may have just been lucky’. We feel that there was significant work involved in balancing the variety of gendered leadership styles within the group. It may be that because this work is seen as selfless and therefore feminine, it is not seen as true work.5
When viewed from an individual’s perspective within the group, gender roles are in fact reinforced by the model itself. Due to the nature of the distribution of tasks, stereotypes are moulded and continually recycled. Rather than challenging their gendered leadership performance participants are comfortable within their gender roles, which are dictated at first by themselves and then perpetuated by the nature of the model.
This comfort acts as an emotive force. We would argue that finding comfort within one’s gendered leadership identity is an important force in the dissipation of anxiety. Participants are not having to perform gender or leadership in a way that feels unnatural or uncomfortable to them, or perform tasks that would otherwise cause stress or anxiety.
We are not suggesting that participants within the group rigidly stuck to the same gendered leadership attributes over the course of the study. The chair (F1), for example, described scenarios where logistically an autocratic stance was the only viable option and thus had to briefly change her leadership performance. F1 has also been noted by members of the group to be able to balance both gendered performances within in short periods of time. Her ability to allow for discussion within the Monday meeting has allowed for the group to develop and foster trust and compassion. Yet M3 noted that F1 was an excellent chair because of her willingness to interrupt, a trait that has been seen by some (and fervently argued against by others) to be masculine.30–32
Furthermore, M4 flitted from a laissez-faire leadership attitude, to being more vocal and engaged within the group. By being responsible for matters regarding the ‘acute floor’, M4 moved away from the reserved figure he portrayed in early meetings, where his greatest contribution had been the rustle of a crisp packet. Likewise M1 showed moments of compassion, which was often met with extreme recognition from colleagues. The reaction to this incongruence displayed by M1 performing feminine leadership, serves as a metaphorical Pandora’s box of leadership behaviours and prejudices, especially when comparing it to the reaction women receive when performing masculine leadership.
Finally when discussing why he believes shared leadership works M3 answered ‘[the participants are] not too rigid in their thinking and are willing to listen’. There must therefore be some malleability in the group’s leadership behaviour to allow for discussion of matters in either a masculine or feminine manner.
Conclusion
This case study has given us some insights into the interplay between gendered leadership and shared leadership. These can be explained on three levels. First, shared leadership (as a whole model) is a feminine model of leadership, with its focus placed on distribution and compassion. Second, because of the disparate behaviours on show, one can argue that the group works on a spectrum of gendered leadership behaviours. The group can be both masculine and feminine, dependent on context. Finally because of this, the model reinforces gendered leadership stereotypes. Participants within a small shared leadership model initially perform gendered leadership in a way that is perceived as natural to the group. This may not be necessarily comfortable to the individual themselves. The shared model subsequently cements these behaviours through its distribution of tasks.
Overall, our case study suggests that for individual participants, shared leadership has not been an opportunity to subvert traditional stereotypes. However, the success of this feminine model may represent a challenge to the prevailing masculine model of leadership within the NHS.
Footnotes
Contributors Both authors contributed to the study design, data analysis and final manuscript. SI-T was responsible for the bulk of the data collection. MA-J drew the comics.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Not required.
Ethics approval Brighton and Sussex University Hospitals Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.