Article Text

Abstract
History suggests that departures from accepted design practice can contribute to positive change in the delivery of mental healthcare, the daily experience of hospitalised patients and public perceptions of mental illness. Yet the question of how architecture can support the therapeutic journey of patients remains a critical one. The availability of evidence-based design literature to guide architects cannot keep pace with growing global demand for new forensic psychiatric hospital facilities. This article reports a global survey of current design practice to speculate on the potential of three new hospitals to positively improve patient experience. A desktop survey was conducted of 31 psychiatric hospitals (24 forensic, 7 non-forensic) constructed or scheduled for completion between 2006 and 2022. This was supplemented by advisory panel sessions with clinical/facilities staff, alongside architectural knowledge obtained through workshops with architects from the UK and the USA, and the inclusion of Australian architects on the research team. Data analysis draws on knowledge from architectural practice, architectural history and environmental psychology, arguing that there is a responsibility to integrate knowledge from across these disciplines in respect of such a pressing and important problem.
- architecture
- cultural history
- mental health care
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The primary method undertaken for this research relied on data publicly available on the internet.
Statistics from Altmetric.com
Introduction
In Australia, the USA and the UK, the number of hospital beds required for forensic mental health treatment doubled between 1996 and 2016.1 Current trends and future predictions suggest this demand will continue to grow. But, in an age where evidence-based practice is highly valued, the demand for new facilities already outpaces the availability of credible evidence to guide designers. This article reports findings from a desktop survey of current design practice across 31 psychiatric hospitals (24 forensic, 7 non-forensic) constructed or scheduled for completion between 2006 and 2022. Desktop surveys, as a form of research, are heavily relied on in architectural practice; photographs and architectural drawings are analysed to understand both typical and innovative approaches to designing a particular building type. While desktop surveys are sometimes supplemented by visits to exemplar projects (which might also be termed ‘fieldwork’), time pressures and budgetary constraints often preclude this. As the result of an academic–industry partnership, the research reported herein embraced practice-based research methods in conjunction with an academic approach. The data set available for the desktop survey was rich but incomplete. Security requirements restrict the public availability of complete floor plans and postoccupancy evaluations. To mitigate these limitations, knowledge was integrated from other disciplines, including environmental psychology, architectural history and professional practice. With regard to the latter, knowledge is specifically around the design and consultation processes that guide the construction of these facilities. This knowledge was used to identify three contemporary hospitals that challenge accepted design practice and, we argue, in doing so have the potential to act as change-agents in the delivery of forensic mental healthcare. We define innovation as variation/s to common, or typical, architectural solutions that can positively improve patients’2 experience of these facilities in ways that directly support one, or a number, of key values underpinning forensic mental healthcare. While this article does not provide postoccupancy data to quantify the value of these innovations, we hope to encourage both designers and researchers to more closely consider these projects—particularly the way that spaces have been designed to benefit patient well-being—and the questions these designs raise for the future of forensic mental healthcare delivery.
Now regarded as naïve is the 19th-century belief that architecture and landscape, if appropriately designed, can restore sanity.3 Yet contemporary research from the field of evidence-based design confirms that the built environment does play a role in the therapeutic process, even if that role does not determine therapeutic outcomes.4 Research regarding the design of forensic mental healthcare facilities remains limited. An article by Ulrich et al recommended that to reduce aggression patients should be accommodated in single rooms; communal areas should have movable furniture; wards should be designed for low social densities; and accessible gardens should be provided.5 An earlier study by Tyson et al showed that lower ward densities can also positively improve patient–staff interactions.6 Commonly, however, the studies referenced above compared older-style mental health units with their contemporary replacements.7 There is little comparative research available that examines contemporary facilities for forensic mental healthcare, with the exception of one article that provided a comparative analysis of nine Swedish facilities, designed between 1990 and 2008.8 However, this article merely described the design aspirations and physical composition of each hospital without investigating the link between design aspiration, patient well-being and the resulting physical environment.
There are two further limitations to evidence-based design research. The first is the extent to which data do not provide directly applicable design tactics. Systematic literature reviews typically provide a set of design recommendations but without suggesting to designers what the corresponding physical design tactics to achieve those recommendations might actually be.9 This is consistent for general hospital design. For example, architects have been advised to provide spaces that are ‘psychosocially supportive’ since 2000, yet it was 2016 before a spatially focused definition of this term was provided, offering designers a more tangible understanding of what they should be aiming for.10 The second limitation is the breadth of research currently available. While rigorous and valuable, evidence-based design often overlooks the fact that architects must design across scales, from the master-planning scale—deciding where to place buildings of various functions within a site, and how to manage the safe movement of staff and patients between those buildings—to the scale of a bathroom door. How do you design a bathroom door to meet antiligature and surveillance requirements, to maintain patient safety, while still communicating dignity and respect for patients? The available literature provides much to contemplate, but in terms of credible evidence much of this research is based on a single study, typically conducted within a single hospital context and often focused on a single aspect of design. This raises the question, is there really a compelling basis for regarding evidence-based design knowledge as more credible than knowledge generated about this building type from other disciplines? In light of the small amount of evidence available in this field, is there not a responsibility to use all the available knowledge?
While the discipline of evidence-based design has existed for three decades,11 purpose-designed buildings for the treatment of mental illness have been constructed for over three centuries. Researchers working within the field of architectural history also understand that patient experience is partially determined—for better or worse—by the decisions that designers make, and that models of care have been used to drive design outcomes since the establishment of the York Retreat in 1796. With their focus on moral treatment, the York Retreat influenced a shift in the way asylum design was approached, from the provision of safe custody to finding architectural solutions to support the restoration of sanity.12 Architectural historians also bring evidence to bear in respect of this design challenge, specifically knowledge of how the best architectural intentions can result in unanticipated (sometimes devastating) outcomes—and of the conditions that gave rise to those outcomes.13 There is a third, rich source of knowledge available to guide designers that, broadly speaking, academic researchers have yet to tap into. It is the knowledge produced by practitioners themselves. Architects learn through experience, across multiple projects and through practice-based forms of enquiry that include desktop surveys (also referred to as precedent studies), user group consultations and gathering (often informal) postoccupancy data from their clients. Architects have already offered a range of tangible solutions to meet particular aspirations related to patient care. There is value in examining these existing design solutions to identify those capable of providing direct benefits to patients that might justify implementation across multiple projects. In understanding how the physical design of forensic psychiatric hospitals can best support the therapeutic journey of patients, all available knowledge should be valued and integrated.
Methodology: embracing ‘mode two’ research
This research was conducted within the context of a master-planning and feasibility study, commissioned by a state government department, to investigate various international design solutions to inform future planning around forensic mental health service provisions in Victoria, Australia. The industry-led nature of this project demanded a less conventional and more inclusive methodological approach. Tight timeframes precluded employing research methods that required ethics approvals (interviewing patients was not possible), while the timeframe and budget precluded the research team from conducting fieldwork. The following obstacles further limited a conventional approach:
Postoccupancy evaluations of forensic psychiatric hospital facilities are seldom conducted and/or not made publicly available.14
Published floor plans that would enable researchers to derive an understanding of the functional layouts and corresponding habits of occupancy within these facilities are limited owing to the security needs surrounding forensic psychiatric hospital sites.
Available literature relevant to the design of forensic psychiatric hospital facilities provides few direct architectural recommendations to offer tactics for how the built environment might support the delivery of treatment.
The team had to find a way to navigate these challenges in order to address the important question of how the physical design of forensic psychiatric hospitals can best support the therapeutic journey of patients.
‘Mode two’ is a methodological approach that draws on the strength of collaborations between academia and industry to produce ‘socially robust knowledge’ whose reliability extends ‘beyond the laboratory’ to real-world contexts.15 It shares commonalities with a phenomenological approach that attributes value to the prolonged, firsthand exposure of the researcher with the phenomenon in question.16 The inclusion of practising architects and academic researchers within the research team provided considerable expertise in the design, consultation and documentation of these facilities, alongside an understanding of the kinds of challenges that arise following the occupation of this building type. Mode two, as a research approach, also recognises that, while architects reference evidence-based design literature, this will not replace the processes through which practitioners have traditionally assembled knowledge about particular building types, predominantly desktop surveys.
A desktop survey was undertaken to understand contemporary design practice within this building type. Forty-four projects were identified as relevant for the period 2006–2022 (31 forensic and 13 non-forensic psychiatric hospitals). These included facilities from the UK, the USA, Canada, Denmark, Norway, Sweden, the United Arab Emirates and Ireland (online supplementary appendix 1). Sufficient architectural information was not available for 13 of these projects and they were excluded from the study. For the remaining 31 facilities, 24 accommodated forensic patients and 7 did not. Non-forensic facilities were included to enable an awareness of any significant programmatic or functional differences in the design responses created for forensic versus non-forensic mental health patients. Architectural drawings and photographs were analysed to identify general trends, alongside points of departure from common practice. Borrowing methods from architectural history, the desktop survey was supplemented by other available information, including a mix of hospital-authored guidebooks (as provided to patients and visitors), architects’ statements, newspaper articles and literature from the field of evidence-based design. Available data varied for each of the 31 hospitals. Adopting a method from architectural theorist Thomas Markus, the materiality and placement of external and internal boundary lines were closely studied (assisted by Google Earth).17 When read in conjunction with the architectural drawings, boundary placement revealed information regarding patient access to adjacent landscape spaces.
Supplemental material
A desktop survey has limitations. It cannot provide a conclusive understanding of how these spaces operate when occupied by patients and staff. While efforts were made to contact individual practices and healthcare providers to obtain missing details, such requests typically went unanswered. This is likely owing to concerns of security, alongside the realities of commercial practice, concerns around intellectual property, and complex client and stakeholder arrangements that can act to prohibit the sharing of this information. To deepen the team’s understanding, a 2-day workshop was hosted to which two international architectural practices were invited to attend, one from the UK and one from the USA. Both practices had recently completed a significant forensic psychiatric hospital project. While neither of these facilities had been occupied at the time of the workshops, the architects were able to share their experiences relative to the research, design, and client and patient consultation processes undertaken. The Australian architects who led the research team also brought extensive experience in acute mental healthcare settings, which assisted in data analysis.
To further mitigate the limitations of the desktop survey, understandings developed by the team were used as a basis for advisory panel discussions with staff. Feedback was sought from five 60 min long, advisory panel sessions, each including four to six clinical/facilities staff (who attended voluntarily during work hours) from a forensic psychiatric hospital in Australia, where several participants recounted professional experience in both the Australian and British contexts. Each advisory panel session was themed relative to various aspects of contemporary design: (1) site/hospital layout, (2) inpatient accommodation, (3) landscape design and access, (4) staff amenities, and (5) treatment hubs (referred to as ‘treatment malls’ in the American context). These sessions enabled the research team to double-check our analysis of the plans and photographs, particularly our assumptions regarding the likely use, practicality and therapeutic value of particular spaces.
Model for analysis
Within general hospital design, a range of indicators are used to measure the contribution of architecture to healing, such as the optimisation of lighting to support sleep, the minimisation of patient falls, or whether the use of single patient rooms assists with infection control.18 In mental health, however, where the therapeutic journey is based more on psychology than physiology, what metrics should be employed to evaluate the success of one design response over another in supporting patient care? We suggest the first step is to acknowledge the values that underpin contemporary approaches to mental healthcare. The second step is to translate those treatment values into corresponding spatial values using a value-led spatial framework.19 This provides a checklist for relating particular spatial conditions to specific values around patient care. For example, if the design intent is to optimise privacy and dignity for patients, then the design of bathrooms, relaxation and de-esculation spaces are all important spaces in respect of that therapeutic value. Highlighting this relationship can assist decision makers to more closely interrogate areas that matter most relative to achieving these values. To put this in context, optimising a bathroom design to prioritise a direct line of sight for staff might improve safety but also obstruct privacy and dignity for patients. While such decisions will always need to be carefully balanced, a value-led spatial framework can provide a touchstone for designers and stakeholders to revisit throughout the design process.
To analyse the 31 projects examined within this project, we developed a framework (Table 1). It recognises that a common approach to patient care can be identified across contemporary Australian, British and Canadian models:
Value-led spatial framework: correlating treatment values with corresponding spaces within the hospital’s physical environment
That patients be extended privacy and dignity to the broadest degree possible without impacting their personal safety or that of other patients or staff.
That patients be treated within the least restrictive environment possible relative to the severity of their illness and the legal (or security) requirements attached to their care.
That patients be afforded choice and independence relative to freedom of movement within the hospital campus (as appropriate to the individual), extending to a choice of social, recreational and treatment spaces.
That patients’ progression through their treatment journey is reflected in the way the architecture communicates to hospital users.
That opportunities for peer-led therapeutic processes and involvement of family and community-based care providers be optimised within a hospital campus. 20
Table 1 assigns a range of architectural spaces and features that are relevant to each of the five treatment values listed. Architectural decisions related to these values operate across three scales: context, hospital and individual. Context decisions are those made in respect of a hospital’s location, including proximity to allied services, connections to public transport and distances to major metropolitan hubs. Decisions of this type are important relative to staffing recruitment and retention, and opportunities for research relative to the psychiatric hospital’s proximity to general (teaching) hospitals or university precincts. Architectural decisions operating at the hospital scale include considerations of how secure site boundaries are provided; how buildings are laid out on a site; and how spatial and functional links are set up between those buildings. This is important relative to the movement of patients and staff across a site, including the location and functionality of therapeutic hubs. But it can also impact patient and community psychology. The design of external fences, in particular, can compound feelings of confinement for patients; focus community attention on the custodial role of a facility over and above its therapeutic function; and influence perceptions of safety and security for the community immediately surrounding the hospital. Architectural decisions operating at the ‘individual’ scale are those that more closely impact the daily experience of a hospital for patients and staff. These include the various arrangements for inpatient accommodation; tactics for providing patients with landscape access and views; and the question of staff spaces relative to safety, ease of communication and collaboration. Approaches to landscape, inpatient accommodation and concerns of staff supervision are closely intertwined.
Findings: what we learnt from 31 contemporary psychiatric hospital projects
Forensic psychiatric hospitals treat patients who require mental health treatment in addition to a history of criminal offending or who are at risk of committing a criminal offence. Primarily, these include patients who are unfit to stand trial and those found not guilty on account of their illness.21 Accommodation is typically arranged according to low, medium or high security needs, alongside clinical need, and whether an acute, subacute, extended or translational rehabilitation setting is required. Security needs are determined based on the risk a patient presents to themselves and/or others, alongside their risk of absconding from the facility. The challenge that has proven intractable for centuries is how can architects balance privacy and dignity for patients, while maintaining supervision for their own safety, alongside that of their fellow patients, the staff providing care and, in some cases, the community beyond.22 In this section we present overall trends regarding the layout of buildings within hospital sites, including the placement of treatment hubs and the design of inpatient wards. Access to landscape is not explicitly addressed in this section but is implicit in decisions around site layout and inpatient accommodation.
Design approaches to site layout
We identified two approaches to site layout—the ‘village’ (4 from 31 hospitals) and the ‘campus’ (27 from 31 hospitals) (figure 1). Similar in their functional arrangement, these are differentiated according to the degree of exterior circulation required to move between patient-occupied spaces. Village hospitals comprise a number of buildings sitting within the landscape, while campus hospitals have interconnected buildings with access provided by internal corridors that prevent the need to go outside. Neither approach is new; both follow the models first used within the 19th century. The village hospital follows the model designed by Dr Albrecht Paetz in 1878 (Alt Scherbitz, Germany), which included detached cottages accommodating patients in groups of between 24 and 100, set within gardens.23 Paetz created this design in response to his belief that upwards of 1000 patients should not be accommodated in a single building, with security measures determined in relation to those patients whose behaviour was the least predictable.24 The resulting monotony of the daily routine and restrictions on patient movement were believed to ‘cripple the intelligence and depress the spirit’.25 Paetz’s model allowed doctors to classify patients into smaller groups and unlock doors to allow patients with predictable behaviour to wander freely within the secure outer boundaries of the hospital.26 This remained the preferred approach to patient accommodation for over a century, as endorsed by the WHO in their report of 1953.27 Broadmoor Hospital (UK, 2019) provides an example of the village model.
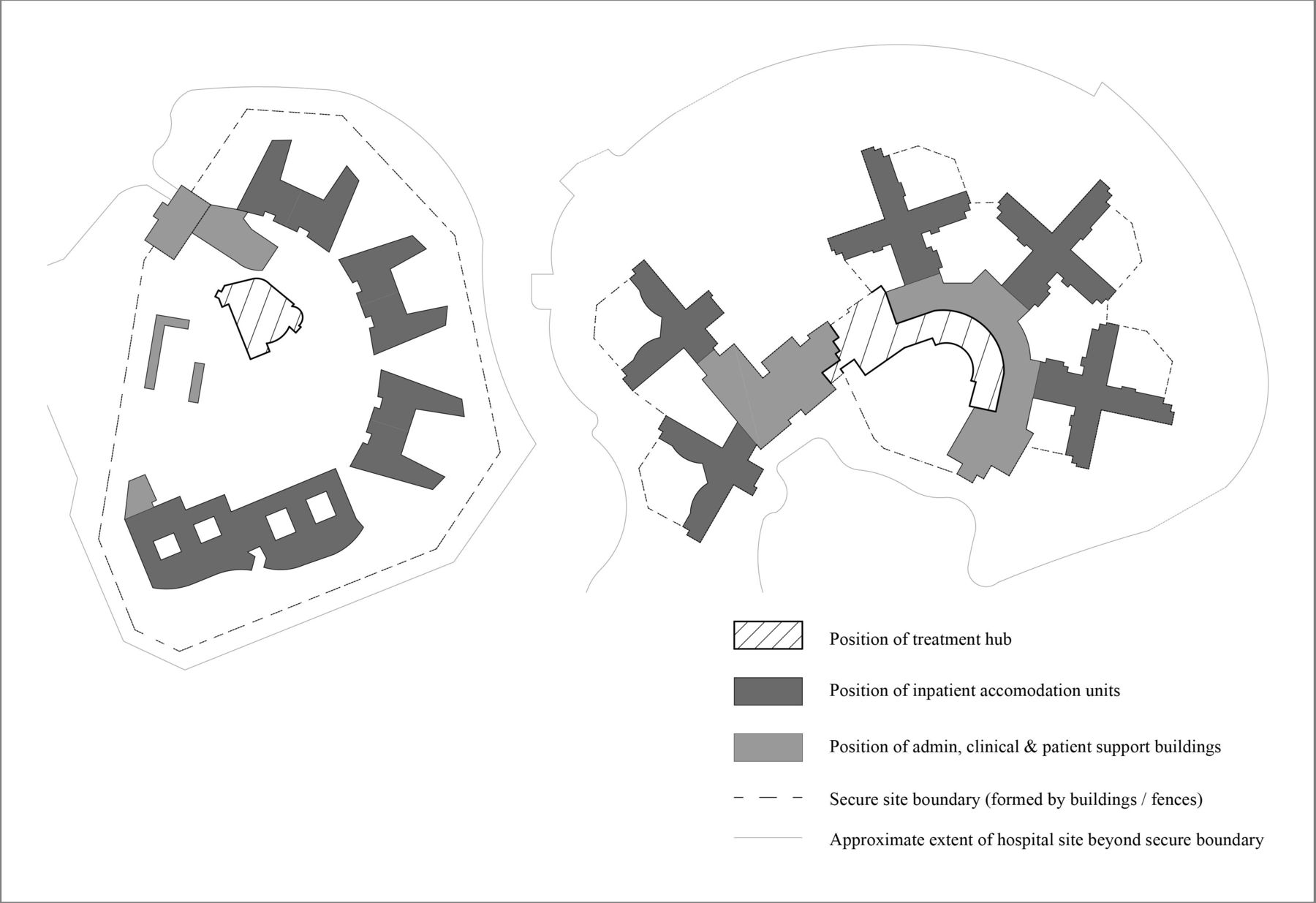
The Broadmoor Hospital (left) follows a ‘village’ arrangement and includes an ‘internal’ treatment hub. The Worcester Recovery Center and Hospital (right) follows a ‘campus’ arrangement and includes an ‘on-edge’ treatment hub.
The campus model is not dissimilar to the approach propagated by Dr Henry Thomas Kirkbride, a 19th-century psychiatrist who was active in the design of asylums and whose influence saw this planning arrangement dominate asylum constructions in the USA for many decades.28 Asylums of the ‘Kirkbride plan’ arranged patient accommodation in a series of pavilions linked by corridors. While corridors can be heavily glazed, where this action is not taken, the campus approach can compromise patient and staff connections to landscape views. Examples of campus hospitals include the Worcester Recovery Center and Hospital (USA, 2012) and the Nixon Forensic Center (USA, under construction).
Treatment hubs are a contemporary addition to forensic psychiatric hospitals. These cluster a range of shared patient spaces, including recreational, treatment and vocational training facilities, and thus drive patient movement around or through a hospital site. Two different treatment hub arrangements are in use: ‘internal’ and ‘on-edge’. Those arranged internally typically place these functions at the heart of the campus and at a significant distance from the secure boundary line. Those arranged on-edge are placed at the far end of campus-model hospitals and, in the most extreme cases, occur adjacent to one of the site’s external boundaries (refer to Figure 1). Both arrangements aspire to make life within the hospital resemble life beyond the hospital as closely as possible, as the daily practice of walking from an accommodation area to a treatment hub mimics the practice of travelling from home to a place of work or study.
With evidence mounting regarding the psychological benefits to patients of landscape access, it should not be assumed that the current preference for campus hospitals over the village model indicates ‘best practice’. A campus arrangement offers security benefits for the movement of patients across a hospital site, while avoiding the associated risks of contraband concealed within landscaped spaces. However, the existence of village hospitals for forensic cohorts suggests it is possible to successfully manage these challenges. Why then do we see such a strong persistence of the campus hospital? This preference may be driven by cultural expectations. From 24 forensic psychiatric hospitals surveyed, 10 were located within the USA and all employed the campus model. Yet nine of those hospitals occupied rural sites where the village model could have been used, suggesting the influence of the Kirkbride plan prevails. The four village hospitals within the broader sample of 31, spanning forensic and non-forensic settings, all occurred within the UK3 and Ireland1. Paetz’s villa model had been the preferred approach to new constructions in these countries since its introduction at close of the 19th century.29 However, a look at UK hospitals in isolation revealed a more even spread of village and campus arrangements, with two of the four UK-based campus hospitals occupying constrained urban sites that required multi-story solutions. The village model would be inappropriate for achieving this as it does not lend well to urban locations where land availability is scarce.
Design approaches to inpatient accommodation
Three approaches to inpatient accommodation were identified: ‘peninsula’, ‘race-track’ and ‘courtyard’ (Figure 2). The peninsula model is characterised by rows of inpatient wings, along a single-loaded or double-loaded corridor that stretches into the surrounding landscape. This typically enables an exterior view from all patient bedrooms and is not dissimilar to the traditional ‘pavilion’ model that emerged within 19th-century hospital design.30 In the racetrack model bedrooms are arranged around a cluster of staff-only (or service) spaces, still enabling exterior views from all patient bedrooms. The courtyard model is similar to the racetrack but includes a central landscape space. Information on the design of inpatient room layouts was available for 24 of the 31 projects analysed (15 of these 24 were forensic).

Common inpatient accommodation configurations. (1) Peninsula: single-loaded version shown (patient rooms on one side only; double-loaded versions have patient rooms on two sides of the corridor); (2) racetrack and (3) courtyard (landscaped). Staff-occupied spaces and support spaces (social space and so on) shown in grey.
Ten forensic hospitals employed a peninsula plan and five employed a courtyard plan. Of the non-forensic psychiatric hospitals five employed the courtyard, three the racetrack and only one the peninsula plan. While the sample size is too small to generalise, the peninsula plan appears to be favoured for a forensic cohort. However, cultural trends again emerge. Of the 10 peninsula plan hospitals, 6 were located within the USA, and among the broader sample of 24 (including the non-forensic facilities) none of the courtyard hospitals were located there. Courtyard layouts for forensic patients occurred within the UK, Ireland, Denmark and Sweden. However, within these countries, a mix of courtyard and peninsula plans were used, suggesting no clear preference for one plan over the other.
Each plan type has advantages and disadvantages (Table 2). Courtyard accommodation provides the following benefits: greater opportunity for patient access to landscape since these are easier for staff to maintain surveillance over; additional safety for staff owing to continuous circulation (staff cannot get caught in ‘dead-ends’; however, the presence of corners which are difficult to see around is a drawback); natural light is more easily available; and ‘swing bedrooms’ can be supported (this is the ability to reconfigure the number of observable bedrooms on a nursing ward by opening and closing doors at different points within a corridor). However, courtyard accommodation requires a larger site area so is better suited to rural locations than urban and is not well suited to multi-story facilities. Peninsula accommodation enables geographical separation, giving medical teams greater opportunity to manage which patients are housed together (‘cohorting’); blind corners can be avoided to assist safety and surveillance; travel distances can be minimised; finally, the absence of continuous circulation provides greater flexibility for creating social spaces for patients with graduated degrees of (semi-)privacy.
Advantages and disadvantages of peninsula versus courtyard accommodation
Another important consideration related to inpatient accommodation is ward size: the number of bedrooms clustered together, alongside the amount of dedicated living space associated with these bedrooms. Ward size can influence patient agitation and aggression, alongside ease of supervision, staff anxiety and safety.31 The most common ward sizes were 24 or 32 beds, further subdivided into subclusters of 8 beds. Typically, each ward was provided with one large living space that all 24 or 32 patients used together. More advanced approaches gave patients a choice of living spaces. For example, at Coalinga Hospital, patients could occupy a small living space available to only 8 patients, or a larger space that all 24 patients had access to. We describe this approach as more advanced since both 19th-century understandings alongside recent research by Ulrich et al confirm that social density (the number of persons per room) is ‘the most consistently important variable for predicting crowding stress and aggressive behaviour’.32 Only six hospitals had plans detailed enough to calculate the square-metre provision of living space per patient, and this varied between 5 and 8 square metres.
Limitations of the desktop survey
Data from a desktop survey are insufficient to obtain a comprehensive understanding of how design contributes to patient experience. To overcome this limitation, the following sections combine knowledge about how people use space from environmental psychology, knowledge about the design and consultation processes that guide the construction of these facilities, and understandings from architectural history. History suggests that seemingly small changes to typical design practice can effect significant change in the delivery of mental healthcare, the daily experience of hospitalised patients and more broadly public perceptions of mental illness. This integrated approach is used to identify three forensic psychiatric hospitals that challenge accepted design practice to varying degrees and, in doing so, have the potential to act as change-agents in the delivery of forensic mental healthcare. But first it is important to understand the context in which architectural innovation is able, or unable, to emerge relative to forensic mental healthcare.
Accepting the challenge: using history to help us see beyond the roadblocks to innovation
Architects tasked with designing forensic mental health facilities respond to what is called a ‘functional brief’; this documents the specific performance requirements of the hospital in question. Much consultation goes into formulating and refining a functional brief through the initial and developed design stages. Consultation is typically undertaken with a variety of different user groups, and in a sequential fashion that includes a greater cross-section of users as the design progresses, including patients, families, and clinical and security staff. Despite the focus on patient experience within contemporary models of care, functional briefs tend to prioritise safety and security, making them the basis on which most major architectural decisions are made.33 In large part this is simply the reality of accommodating a patient cohort who pose a risk of harm towards themselves and/or others. A comment from Tom Brooks-Pilling, a member of the design team for the Nixon Forensic Center (Fulton, Missouri), provides insight into this approach and the concerns that drive it. He explained that borrowing a ‘spoked wheel’ arrangement from prison design eliminated blind spots and hiding places to enable a centrally located staff member to:
see everything that’s going on in that unit…[they are] basically watching the other staff’s back [sic] to make sure that they can focus on treatment and not worry about who might be sneaking up on them or what activities might be going on behind their backs.34
Advisory panel feedback confirmed that when the architectural design of a facility heightens staff anxiety this has direct ramifications for the therapeutic process. For example, in spaces where staff could become isolated from one another, and where clear lines of sight were obstructed, such as ill-designed elevators or stairwells, this can lead to movement being reduced across the patient cohort to avoid putting staff in those spaces where they feel unsafe.
The architects consulted during the course of this research, including those who were part of the research team, articulated how the necessary prioritisation of safety, in turn, leads to compromises in the attainment of an ideal environment to support treatment. In the various forensic and acute psychiatric hospital projects they had been involved with, all observed a sincere commitment on the part of those engaged in project briefing to upholding ideals around privacy, dignity, autonomy and freedom of movement for patients. They reported, however, that the commitment to these ideals was increasingly obstructed as the design process progressed by the more pressing concerns of safety. Examples of the kinds of architectural implications of this prioritisation are things like spatially separated nursing stations (enclosed, often fully glazed), when a desire for less-hierarchical interactions between patients and staff had been expressed at the beginning of the briefing process; or the substitution of harder-wearing materials, with a more ‘institutional’ feel when a ‘home-like’ atmosphere had been prioritised initially. There is nothing surprising or unusual about this process since design is, by its nature, a process of seeking improvements on accepted practice while systematically checking the suitability of proposed solutions against a set of performance requirements. In the context of forensic psychiatric hospitals, safety is the performance requirement that most often frustrates the implementation of innovative design. Thus, amid the complexities of design and procurement relative to forensic psychiatric hospitals, innovation, however humble, and particularly where it can be seen to contribute positively to the patient experience, is worth a closer look.
In the historical development of the psychiatric hospital as a building type, two significant departures from accepted design practice facilitated positive change in the treatment of mental illness. The first was Paetz’s development of the village hospital which sought to replace high fences, locked doors and barred windows with ‘humane but stringent supervision’.35 While this planning approach may not have significantly altered models of care, it was regarded as ‘an essential, vital development’, providing architectural support to the prevailing approach to treatment of the time—that of moral treatment—which aimed to extend kindness and respect to patients, in an environment that was as unrestrictive as possible. The York Retreat is worthy of acknowledgement here as a leading proponent of moral treatment whose influence shifted approaches to asylum design, from focusing on the provision of safe custody to supporting the restoration of sanity. Architecturally, however, the differences in the York Retreat’s approach were mainly focused on interior details that encouraged patients to maintain civil habits. Dining rooms had white tablecloths and flower vases adorned mantelpieces, door locks were custom-made to close quietly, and window bars fashioned to look like domestic window frames.36 The York Retreat was originally a small institution, in line with Samuel Tuke’s preference for a maximum asylum size of 30 patients. History confirms the extent to which this approach was not scalable and thus unable to be replicated widely for asylum construction. For these reasons, it has not been considered here as a significant departure from accepted design practice.
The second significant departure from accepted design practice was the development of acute treatment hospitals, located within cities, adjacent to general hospitals and medical research facilities. The first hospital of this type was the Maudsley Hospital, led by doctors Henry Maudsley and Frederick Mott, in London. The design intent for this hospital was announced in 1908 but it was not opened until 1923.37 In proposing this hospital, Maudsley and Mott were motivated to bring psychiatry ‘into line with the other branches of medical science’.38 This 100-bed facility, located directly across the road from the King’s College (Teaching) Hospital, emulated the general hospital typology in offering both outpatient and short-duration inpatient care, specifically targeted at patients with recent-onset illnesses. The aspirations were threefold: to avoid the stigma associated with large public asylums; to advance the medical understanding of mental illness through research collaborations with general hospitals and medical schools and via improved teaching programmes; and to both enable and encourage patients to access early, voluntary treatment on an outpatient basis.38 Today the Maudsley appears unremarkable, an unassuming three-storied building on a busy London street. But the significance of what this building communicated at the time it was constructed, and the extent to which it challenged accepted practice, should not be underestimated. The Maudsley sent a clear message to the public that mental illness was no longer to be regarded as different from any other illness treated within a general hospital setting; that it was no longer okay to isolate those suffering from mental illness from their families or the neighbourhoods in which they lived.39 Following the announcement of the Maudsley, the ‘psychopathic hospital’ rose to prominence within the USA with Johns Hopkins University Hospital opening the Phipps Psychiatric Clinic, in Baltimore, in 1913. The psychopathic hospital similarly promoted urban locations and closer connections to teaching and research. The Maudsley can be seen to have played a significant role in the shift to treating acute mental illness within general hospital settings.
In any discussion of the history of institutional care, there is a responsibility to acknowledge that the aspiration to provide buildings that support care and recovery have not always manifested in ways that improved daily life for patients. The five treatment values that underpinned the analysis framework for this project are not new values. The extension of privacy and dignity to patients and the delivery of care within the least restrictive environment possible were both firmly embedded in the 19th-century approach of moral treatment. Yet the rapid growth of asylum care frustrated the delivery of those values to patients.40 Choice and independence for patients, the desire for a patient’s recovery progress to be reflected in their environment, and opportunities for peer support and family involvement have been present in approaches to mental health treatment since the formal endorsement of the ‘therapeutic community’ approach to hospital construction and administration in the WHO’s report of 1953.41 History reminds us, therefore, that differences can arise between the stated values on which an institution is designed and those which it is constructed and operated. The three hospitals discussed in the following section include innovative solutions that hold the promise of positive benefits for patients. Yet we acknowledge this a theoretical analysis. For concrete evidence of a positive relationship between these design outcomes and patient well-being, postoccupancy evaluations are required.
Three hospitals contributing to positive change in forensic mental healthcare
Broadmoor Hospital: optimising the value of the village model for patients
Nineteenth-century beliefs and contemporary research are in accord regarding the importance of greenspace in reducing agitation within forensic psychiatric hospital environments and in promoting positive patterns of socialisation.42 It is surprising, therefore, that enshrining daily landscape access for patients is not widespread within current design practice. The Irish National Forensic Mental Hospital and the State Hospital at Carstairs (Scotland) both follow the model of the village hospital, but only in that they comprise a number of accommodation buildings set within the landscape, enclosed by an external boundary fence. At the Irish National Forensic Mental Hospital, the scale of the landscape—the distance between buildings and the lack of intermediate boundaries within the landscape—suggests it is highly unlikely that patients are allowed to navigate this landscape on a regular basis. By comparison, the architectural response developed for Broadmoor Hospital (2019) shows an exemplary commitment to patient views and access to landscape (Figure 3).

Likely extent of landscape occupation by patients as indicated by the position of inner and outer secure boundary lines. (1) Broadmoor Hospital (rural site, UK), (2) Irish National Forensic Mental Hospital (rural site) and (3) Roseberry Hospital (suburban site, UK).
Five contemporary hospitals follow the logic of a traditional villa hospital, yet Broadmoor is the only one that optimises the benefits offered by this spatial configuration. Comprising a gateway building and a central treatment hub, with a series of patient accommodation buildings positioned around it, the landscape becomes the only available circulation route for patients travelling off-ward to the shared therapy, recreation and vocational training spaces. Most patients will thus engage with the outdoors at least twice daily on their way to and return from these shared spaces. But in addition to accessing this central landscape, landscape views from patient rooms have been prioritised, and each ward is allocated its own large greenspace. Multiple, internal boundary fences enable patient access to the adjacent landscape to the greatest possible degree (refer to Figure 3). This approach provides patients with a diversity of landscape experiences. This is important given the patterns of landscape use between forensic and non-forensic hospitals. In non-forensic facilities, patients are likely to have the choice of accessing multiple landscape spaces, whereas in forensic facilities access to a particular space is often restricted to one cohort, for example, a single ward group. This highlights a limitation of the courtyard model for forensic patients. Roseberry Park Hospital (2012) provides an example of how a high degree of landscape access can be similarly achieved for patients on constrained urban site, using a courtyard layout (refer to Figure 3).
Providing patients with daily landscape access provides challenges to maintaining safety and security. Trees with low branches can be used as weapons, while tall branches can be used for self-harm, and ground cover landscaping increases opportunities to conceal contraband. At the Australian hospital where advisory panel sessions were conducted (constructed in 2000), the landscape is occupied in a similar way and staff conveyed the constant effort required to ensure safe patient access to this greenspace. Significant costs are incurred annually by facilities staff in keeping the greenspace free from contraband and from several varieties of wild mushroom that grow seasonally on the site. Despite this cost, staff reported that both they and the patients value the opportunity to circulate through the landscaped grounds (even in inclement weather); hence, the benefits to well-being are perceived as significant enough to justify this cost. These examples make evident that placing a hospital within a landscape is not enough to ensure patients are extended the well-being benefits of ongoing access. Instead this requires that hospitals factor in the additional supervisory and maintenance requirements to maintain landscape access for patients.
Worcester Recovery Center and Hospital: spaces to support choice and a sense of control
Research in environmental psychology, conducted within residential and hospital settings, confirms that the ability to regulate social contact can have a dramatic impact on well-being. The physical layout of spaces has been linked to both the likelihood of developing socially supportive relationships and impeding this development, with direct implications for communication, concentration, aggression and a person’s resilience to irritation.43 These problems can be more pronounced in a forensic psychiatric hospital as there is an over-representation of patients who have suffered trauma. Architects working in forensic psychiatric hospital design acknowledge that patients need space to withdraw from the busy hospital environment, spaces where they can ‘observe everything that is going on around them until they feel ready to join in’.44 It is surprising, therefore, that many contemporary forensic psychiatric hospitals still continue to provide a single social space for all 24 or 32 patients occupying a ward. The Worcester Recovery Center, by comparison, provides patients with a choice of social spaces that are designed to enable graduated degrees of social engagement. This can support a sense of control to limit socially induced stress.
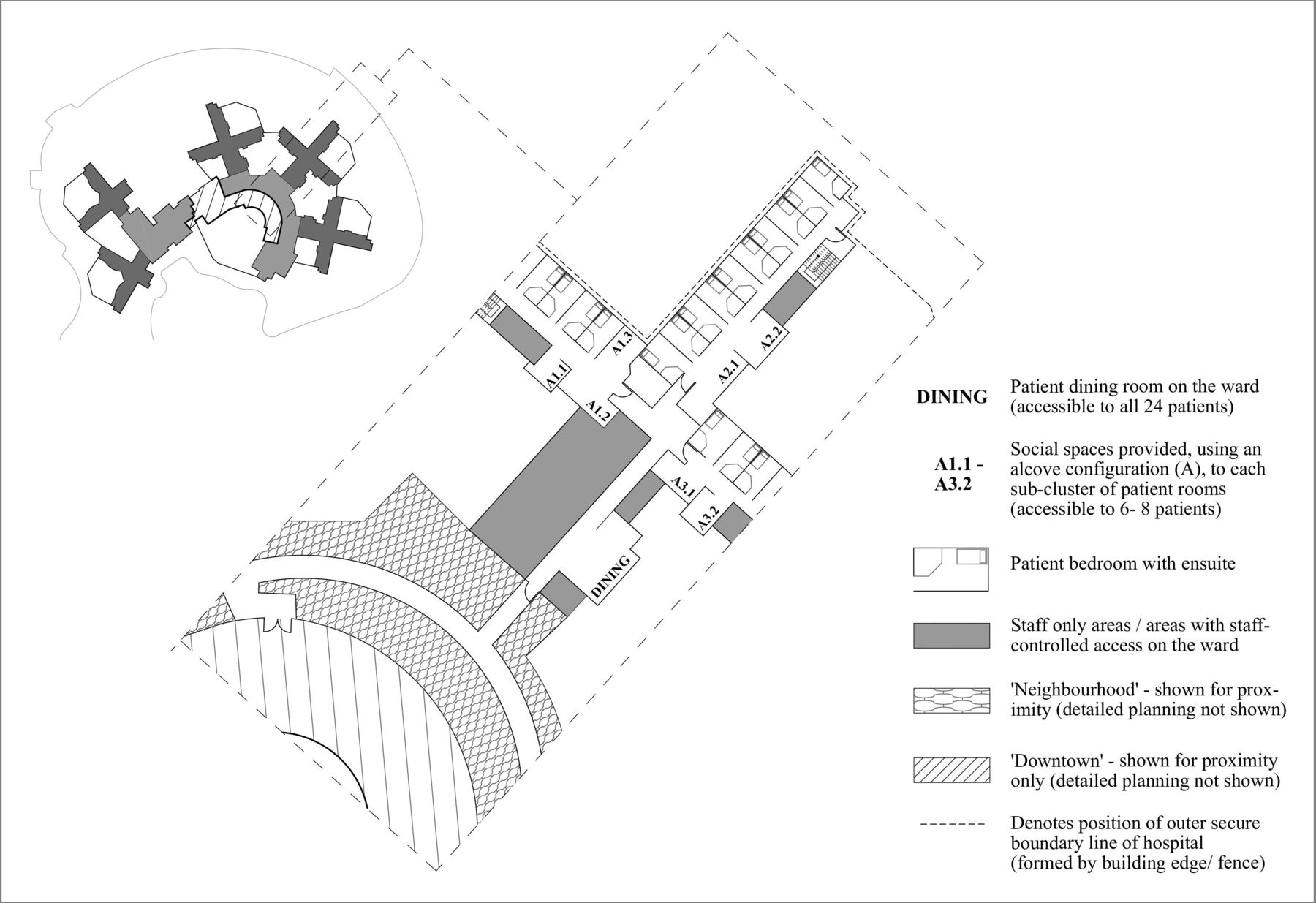
Worcester is conceptualised as three distinct zones designed to resemble life beyond the hospital: the ‘house’, ‘neighbourhood’ and ‘downtown’ (Figure 4). The house zones include patient accommodation, employing a peninsula model. Each comprises 26 patient rooms, clustered into groups of 6 or 10 single bedrooms that face a collection of shared spaces dedicated to that cluster, including sitting areas, lounges and therapeutic spaces. A shared kitchen and dining room is provided for each house. Three houses feed into a neighbourhood zone that includes shared spaces for therapy and vocational training, while the downtown zone serves a total of 14 houses. The downtown zone can be accessed by patients based on a merit system and includes a café, bank and retail spaces, music room, health club, chapel, green house, library and art rooms, alongside large interior public spaces. This array of amenities does not seem distinctly different from other contemporary facilities, where therapy and vocational training happen in a mix of on-ward and off-ward (often within a central treatment hub). The difference lies in the sensitivity of how these spaces are articulated.
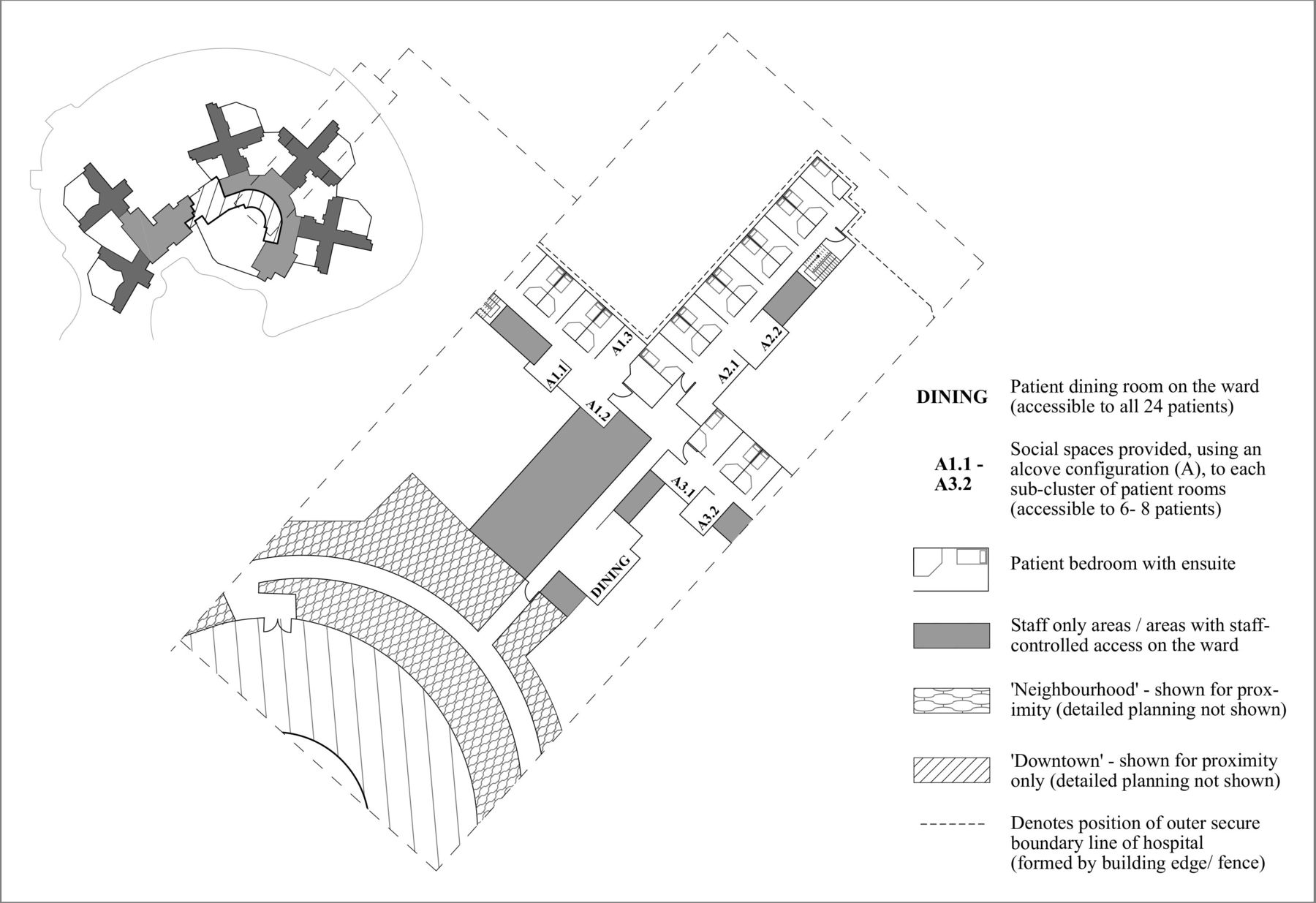
Details of the social spaces provided on each ward at the Worcester Recovery Center and the proximity of the ‘house’ (or ward) to the ‘neighbourhood’ and ‘downtown’.
The generosity of providing separate living spaces for every 6–10 patients and locating these directly across the corridor from the patient rooms supports a sense of control and choice for patients. Frank Pitts, an architect who worked on the Worcester project, has written that this was done to enable patients to ‘decide whether they are ready to step out and socialise or return to the privacy of their room’.45 This approach filters throughout the facility, providing a slow graduation of social engagement opportunities for patients, from opportunities to socialise with their cluster of 6–10 individuals, to their house of 26, to their neighbourhood of 78 people, to the full downtown experience. According to the architects, the neighbourhood thus provides an intermediary zone between the quiet house and the active downtown, which can be overwhelming for some patients.46 Importantly the scale of the architecture responds to this transition from personal to public space, providing visual indicators to reflect patients’ movement through their treatment journey; spaces become larger as they move further from the ward. This occurs because instead of providing a single, large shared living space, patients are provided a choice of smaller spaces to occupy—these are not much bigger than a patient bedroom. Dining spaces are slightly larger, while downtown spaces have a civic quality; these are double-height, providing a greater sense of light and airiness. These are arranged in a semicircle, opening onto a large veranda and greenspace. The sensitive articulation of these spaces, with regard to both their graduated physical scale and the proximity of the social spaces to the patient bedrooms, provides spatial support to these social transitions while empowering patients to control their own level of social interaction.
Margaret and Charles Juravinski Centre for Integrated Healthcare: creating opportunities for greater public engagement and supporting readjustment to the world beyond the hospital
One of the most significant barriers to mental health treatment is the stigma associated with admission to a psychiatric hospital. We know that discrimination poses an obstacle to recovery and that the media fuels public fears related to forensic mental health patients.47 Two further challenges to mental health delivery include the disconnection patients can experience from the community, including from family and educational opportunities, and the risk of readmission in the period immediately following discharge.48 If architecture is capable of acting as a change-agent in the delivery of mental healthcare, then it needs to show leadership, not only in the provision of a better experience for patients but more broadly in taking steps to help shift public perceptions around mental illness. The Margaret and Charles Juravinski Centre for Integrated Healthcare (MCJC) (Canada) displays several similarities with the approach taken to the Maudsley Hospital. Its appearance communicates a modern, cutting-edge healthcare facility; it does not hide on a rural site or behind walls. At five stories, and extensively glazed, MCJC communicates a strong civic presence. Its proximity to McMaster University (6 km) and to neighbouring general hospitals, including Juravinski Hospital (4 km) and Hamilton General Hospital (4 km), positions it well for research collaborations to occur, while its proximity to the Mohawk Community College, across the road, can enable patients with leave privileges to access vocational training. More importantly, it employs three innovative design tactics to target the challenges of contemporary forensic mental healthcare, providing an example for how architecture might broker positive change.
The first innovative design strategy is the co-location of support services for outpatient mental healthcare. The risk of readmission is highest immediately following discharge. A lack of collaboration between outpatient support services can result in fragmented care when patients are most vulnerable to the stresses associated with readjustment to the world beyond.49 MCJC includes outpatient facilities allowing patients to use the hospital as a stable base, or touchstone, in adjusting to life after discharge. Bringing these services onto the same physical site can also improve opportunities for coordination between inpatient and outpatient support services which can support continuity of care. The second design strategy is the co-location of a medical ambulatory care centre which includes diagnostic imaging, educational and research facilities. This creates reasons for the general public to visit this facility, setting up the opportunity for greater public interaction. This could potentially advance understandings of the role of this facility and the patients it treats.
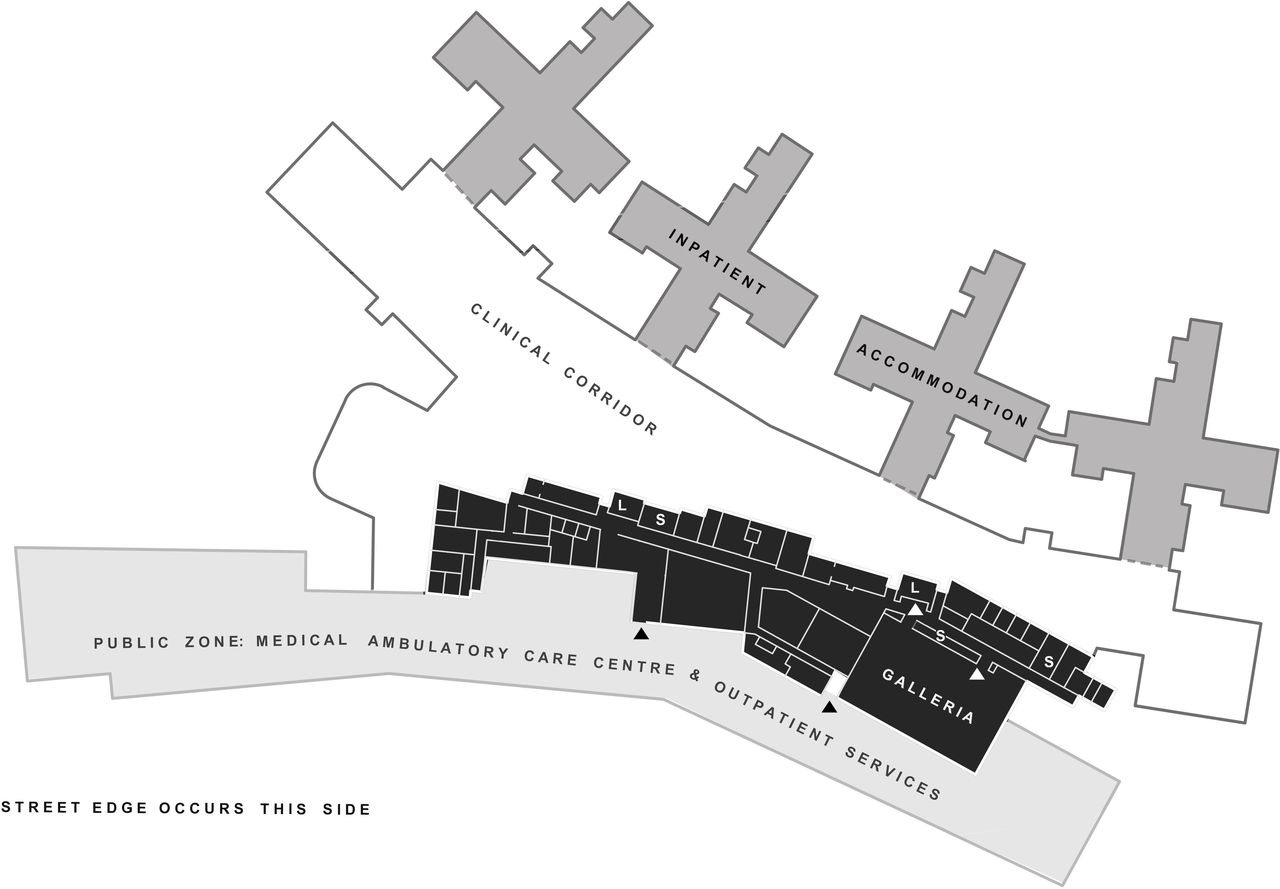
The third innovative design strategy was to optimise the on-edge treatment hub for public engagement. While adopted across a number of hospitals, including Hawaii State Hospital, Helix Forensic Psychiatry Clinic (Sweden) and the Worcester Recovery Center, the on-edge treatment hubs at these hospitals are buried deep inside the secure outer boundary. At MCJC, the treatment hub is placed adjacent to the public zones of the hospital—although on the second floor—and this can be viewed as extension of the public realm and enables the potential for the public to be brought right up to the secure boundary line (which occurs within the building). MCJC is divided into four zones: the public zone, the galleria (the name given to the treatment hub), the clinical corridor and inpatient accommodation (Figure 5). The galleria functions similarly to the downtown at the Worcester Recovery Center; patients are given graduated access to a series of spaces that support their recovery journey. These include a gym, wellness centre, spiritual centre, library, café, beauty salon, and retail and financial services, alongside patient and family support services. While the galleria was initially intended to be accessible by the general public, this was not immediately implemented on the facilities’ opening and it is unclear whether this has now occurred.50 Nonetheless, the potential for movement of patients outwards, and families inwards, has been built into the physical fabric of this building, meaning opportunities for social interaction and fostering greater public understanding are possible. If understanding is the antidote to discrimination, then exposing the public to the role of this facility and the patients it treats is an important step in the right direction.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Zoning configuration at the Margaret and Charles Juravinski Centre for Integrated Healthcare. The galleria zone is on the second floor (shown in black). The arrows indicate main access points to the galleria. Lifts (L) and stairwell (S) positions are indicated.
Conclusion
The question of how architecture can support the therapeutic journey of forensic mental health patients is a critical one. Yet the availability of evidence-based design literature to guide designers cannot keep pace with growing global demand for new forensic psychiatric hospital facilities, while limitations remain relative to the breadth and usability of this research. A narrow view of what constitutes credible evidence can overlook the value of knowledge embedded in architectural practice, alongside that held by architectural historians and lessons from environmental psychology. In respect of such a pressing and important problem, there is a responsibility to integrate knowledge from across these disciplines. Accepting the limitations of a theoretical analysis and of the desktop survey method, we also argue for its value. Architects learn through experience, across multiple projects. This gives weight to the value of examining existing, contemporary design solutions to identify architectural innovations capable of providing benefits to patients and thus perhaps worthy of implementation across multiple projects. History gives us reason to believe that small changes to typical design practice can improve the delivery of mental healthcare, the daily experience of hospitalised patients and more broadly public perceptions of mental illness. Architecture has the capacity to contribute to positive change.
Here, we have provided a nuanced way for architects and decision makers to think about the relationship between architectural space and treatment values. An institution’s model of care and the therapeutic values that underpin that model of care should be placed at the centre of architectural decision making. A survey of contemporary architectural solutions confirms that, generally speaking, innovation is lacking in this field. There will always be real obstacles to innovation, and the argument presented here does not suggest it is necessarily practical to prioritise therapeutic values at the cost of patient, staff and community safety. Instead, it challenges architects and decision makers to properly interrogate any architectural decision that compromises an initial commitment to supporting a patient’s treatment journey—to be more idealistic in the pursuit of positive change.
Tangible examples exist of architectural innovations capable of positively improving patient experience by supporting key values that underpin contemporary treatment approaches. The Broadmoor Hospital optimises the value of the village model for patients, prioritising patient needs for frequent landscape engagement to support their therapeutic journey. The Worcester Recovery Center provides a generous choice and graduation of social spaces to support the social reintegration of patients at their own pace. MCJC co-located facilities to support a patient’s readjustment to daily life postdischarge, while creating opportunities for public engagement that has the potential to foster greater public understanding of the role of these institutions and the patients they treat. In identifying these three innovative design approaches, we provide architects with tangible design tactics, while encouraging researchers to look more closely at these examples with targeted, postoccupancy studies. These projects provide hope that with a shared vision and commitment, innovation is possible in forensic psychiatric hospital design, with tangible benefits for patients.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The primary method undertaken for this research relied on data publicly available on the internet.
Ethics statements
Patient consent for publication
Acknowledgments
The opportunity to conduct this project arose out of a multidisciplinary master-planning and feasibility study, commissioned by the Victorian Health and Human Services Building Authority, to investigate various international solutions to inform future planning and design around forensic mental health service provision. The following people contributed their time and expertise in shaping the research process that enabled this article: Neel Charitra, Stefano Scalzo, Les Potter, Margaret Grigg, Lousie Bawden, Matthew Balaam, Martin Gilbert, John MacAllister, Crystal James, Jo Ryan, Julie Anderson, Jo Wasley, Sophie Patitsas, Meagan Thompson, Judith Hemsworth, James Watson, Viviana Lazzarini, Krysti Henderson, Nadia Jaworski, Jack Kerlin and Jan Merchant.
Notes
1. Jamie O'Donahoo and Janette Graetz Simmonds (2016), “Forensic Patients and Forensic Mental Health in Victoria: Legal Context, Clinical Pathways, and Practice Challenges,” Australian Social Work 69, no. 2: 169–80.
2. The challenge of which terminology to select when writing about psychiatric hospital design remains difficult relative to the stigmas that surround this field. The term ‘patient’ has been used throughout, instead of ‘consumer’, as this article spans both historical and contemporary developments. In the context of this timespan, consumer is a relatively recent term, introduced around 1985.
3. B Edginton (1994), “The Well-Ordered Body: The Quest for Sanity through Nineteenth-Century Asylum Architecture,” Canadian Bulletin of Medical History 11, no. 2: 375–86; Clare Hickman (2009), “Cheerful Prospects and Tranquil Restoration: The Visual Experience of Landscape as Part of the Therapeutic Regime of the British Asylum, 1800-60,” History of Psychiatry 20, no. 4 Pt 4: 425–41; Rebecca McLaughlan, 2012), “Post-Rationalisation and Misunderstanding: Mental Hospital Architecture in the New Zealand Media,” Fabrications 22, no. 2: 232–56.
4. Roger S Ulrich et al. (2008), “A Review of the Research Literature on Evidence-Based Healthcare Design,” HERD 1, no. 3: 61–125; Jill Maben et al. (2015), “Evaluating a Major Innovation in Hospital Design: Workforce Implications and Impact on Patient and Staff Experiences of All Single Room Hospital Accommodation,” Health Services and Delivery Research 3: 1–304; Penny Curtis and Andy Northcott (2017), “The Impact of Single and Shared Rooms on Family-Centred Care in Children’s Hospitals,” Journal of Clinical Nursing 26, no. 11–12: 1584–96.
5. Roger S. Ulrich et al. (2018), “Psychiatric Ward Design Can Reduce Aggressive Behavior,” Journal of Environmental Psychology 57: 53–66.
6. Graham A Tyson, Gordon Lambert, and Lyn Beattie (2002), “The Impact of Ward Design on the Behaviour, Occupational Satisfaction and Well-Being of Psychiatric Nurses,” International Journal of Mental Health Nursing 11, no. 2: 94–102.
7. For further examples of this see Jon E. Eggert et al. (2014), “Person-Environment Interaction in a New Secure Forensic State Psychiatric Hospital,” Behavioral Sciences & the Law 32, no. 4: 527–38; C.C. Whitehead et al. (1984), “Objective and Subjective Evaluation of Psychiatric Ward Redesign,” The American Journal of Psychiatry 141, no. 5: 639–44; Gabriela Novotná et al. (2011), “Client-Centered Design of Residential Addiction and Mental Health Care Facilities: Staff Perceptions of Their Work Environment,” Qualitative Health Research 21, no. 11: 1527–38.
8. Morgan Andersson et al. (2013), “New Swedish Forensic Psychiatric Facilities: Visions and Outcomes,” Facilities 31, no 1/2: 24–88.
9. For examples see Kathleen Connellan et al. (2013), “Stressed Spaces: Mental Health and Architecture,” HERD: Health Environments Research & Design Journal 6, no. 4: 127–168; Constantina Papoulias et al. (2014), “The Psychiatric Ward as a Therapeutic Space: Systematic Review,” British Journal of Psychiatry 205, no. 3: 171–6.
10. R. Allen and R.G. Nairn, 1997; Alan Dilani, 2000, “Psychosocially Supportive Design - Scandinavian Health Care Design,” World Hospitals and Health Services 37: 20–4; Rebecca McLaughlan (2018), “Psychosocially Supportive Design: The Case for Greater Attention to Social Space within the Pediatric Hospital," HERD 11, no. 2: 151–62.
11. Rebecca McLaughlan (2017), “Learning From Evidence-Based Medicine: Exclusions and Opportunities within Health Care Environments Research,” Design for Health 1: 210–28.
12. B Edginton (1997), “Moral Architecture: The Influence of the York Retreat on Asylum Design,” Health & Place 3, no. 2: 91–9; Jeremy Taylor (1991), Hospital and Asylum Architecture in England 1849–1914: Building for Health Care (London: Mansell Publishing Limited); Anne Digby (1985), Madness, Morality and Medicine: A Study of the York Retreat 1796–1914 (New York: Cambridge University Press).
13. Digby, Madness, Morality and Medicine; Erving Goffman (1961), Asylums: Essays on the Social Situation of Mental Patients and Other Inmates (New York: Doubleday); Ivan Belknap (1956), Human Problems of a State Mental Hospital (New York: Blakiston Division, McGraw-Hill); Andrew Scull (1979), Museums of Madness: The Social Organization of Insanity in 19th Century England (London: Allen Lane); Leonard Smith (1999), Cure, Comfort and Safe Custody: Public Lunatic Asylums in Early Nineteenth-Century England (London: Leicester University Press); Rebecca McLaughlan (2014), “One Dose of Architecture, Taken Daily: Building for Mental Health in New Zealand” (PhD diss., Victoria University of Wellington, New Zealand).
14. Although not fitting a strict definition of postoccupancy evaluation, the following articles were notable exceptions to this finding: Eggert et al., “Person-Environment Interaction,” 527–38; Roger S. Ulrich et al. (2018), “Psychiatric Ward Design Can Reduce Aggressive Behavior,” 53–66; Catherine Clark Ahern et al. (2016), “A Recovery-Oriented Care Approach: Weighing the Pros and Cons of a Newly Built Mental Health Facility,” Journal of Psychosocial Nursing and Mental Health Services 54, no. 2: 39–48.
15. M Gibbons (2000), “Mode 2 Society and the Emergence of Context-Sensitive Science,” Science and Public Policy 27: 161.
16. D Seamon, 2000, “A Way of Seeing People and Place,” in Theoretical Perspectives in Environment-Behavior Research, ed. S. Wapner, J. Demick, T. Yamamoto and H. Minami (New York: Plenum), 157–78.
17. Thomas A Markus (1982), Order in Space and Society: Architectural Form and Its Context in the Scottish Enlightenment (Edinburgh: Mainstream Publishing Company).
18. Ulrich et al., “A Review of the Research Literature,” 61–125.
19. This was first created by first author for use for historical analysis during her PhD and is applied here to a contemporary setting. Refer to McLaughlan, “One Dose of Architecture, Taken Daily.”
20. The following documents were referenced in compiling this list: Joint Commission Panel for Mental Health, NHS, UK (2013), “Guidance for Commissioners of Forensic Mental Health Services,” May, https://www.jcpmh.info/resource/guidance-for-commissioners-of-forensic-mental-health-services/; Cannon Design (2014), “St Joseph’s Integrated Healthcare Hamilton, Margaret and Charles Juravinski Centre for Integrated Healthcare,” Healthcare Design Showcase, September; Health Nexus Group, 2017, “Forensicare Model of Care Report,” April, Australia (access provided by the Victorian Health and Human Services Building Authority); Donald Cant Watts Corke (2014), “Service Plan for Forensic Mental Health Services,” July, Australia (access provided by the Victorian Health and Human Services Building Authority).
21. Sometimes this includes patients with no history of criminal behaviour but who are unable to be treated safely in a general hospital environment.
22. W.A.F Browne (1991), "What Asylums Were, Are and Ought to Be (1837),” reprinted in The Asylum as Utopia: W.A.F. Browne and the Mid-Nineteenth Century Consolidation of Psychiatry, ed. Andrew Scull (London: Tavistock); Morgan Andersson et al. (2013), “New Swedish Forensic Psychiatric Facilities,” 24–38; Eggert et al., “Person-Environment Interaction.”
23. Anon (1895), “Review: The Colonization of the Insane in Connection with the Open-Door System: Its Historical Development and the Mode in Which It Is Carried Out at Alt Scherbitz Manor. By Dr. Albrecht Paetz, Director of the Provincial Institution for the Insane (Berlin: Springer, 1983),” The Journal of Mental Science 41: 697–703.
24. Theodore Gray (1958), The Very Error of the Moon (Ilfracombe & Devon: Arthur H. Stockwell Ltd), 64.
25. John Galt (1854), “The Farm of St. Anne,” American Journal of Insanity II (1854): 352.
26. Galt, “The Farm of St. Anne,” 352.
27. Martin James (1948), “Diagnostic Measures,” in Modern Trends in Psychological Medicine, ed. Noel Haris (London: Buttefwork & Co. Ltd), 146; World Health Organization (1953), The Community Mental Hospital: Third Report of the Expert Committee on Mental Health (Geneva: WHO).
28. Carla Yanni (2007), The Architecture of Madness: Insane Asylums in the United States. Minneapolis (London: University of Minnesota Press).
29. Key British examples included the 1923 rebuild of London’s Bethlem Hospital which followed the villa model, alongside Shenley Park Mental Hospital (Middlesex County) and Barrow Mental Hospital (Somerset), both constructed in the early 1930s.
30. Taylor, Hospital and Asylum Architecture in England.
31. Ulrich et al., “Psychiatric Ward Design Can Reduce Aggressive Behavior,” 53–66; O. Jenkins, S. Dye and C. Foy (2015) (Oliver Jenkins et al., 2015), “A Study of Agitation, Conflict and Containment in Association With Change in Ward Physical Environment,” Journal of Psychiatric Intensive Care 11, no. 01: 27–35; M. Daffern, M.M. Mayer, and T. Martin (2004), “Environmental Contributors to Aggression in Two Forensic Psychiatric Hospitals,” International Journal of Forensic Mental Health 3 no. 1: 105–114; Kathryn L. Brooks et al. (1994), “Patient Overcrowding in Psychiatric Hospital Units: Effects on Seclusion and Restraint,” Administration and Policy in Mental Health 22, no. 2: 133–44; T. T Palmstierna, B Huitfeldt, and B Wistedt (1991), “The Relationship of Crowding and Aggressive Behavior on a Psychiatric Intensive Care Unit,” Psychiatric Services 42, no. 12: 1237–40.
32. Ulrich et al., “Psychiatric Ward Design Can Reduce Aggressive Behavior,” 57; Charles Mercier (1894), Lunatic Asylums: Their Organisation and Management (London: Charles Griffin and Company), 135.
33. Morgan Andersson et al. (2013), “New Swedish Forensic Psychiatric Facilities,” 24–38; Joel A Dvoskin et al. (2002), “Architectural Design of a Secure Forensic State Psychiatric Hospital,” Behavioral Scients & the Law, 20, no. 3: 481-493; J. Enser and D. Maclnnes (1999), “The Relationship between Building Design and Escapes from Secure Units,” Journal of the Royal Society for the Promotion of Health 119, no. 3: 170–4; Jon E. Eggert et al. (2014), “Person-Environment Interaction,” 527–38.
34. Tom Brooks-Pilling cited in Mike Lear (2015), “Designer: New Fulton State Hospital Will Be Better, Safer,” Missourinet, January 5, https://www.missourinet.com/2015/01/05/designer-new-fulton-state-hospital-will-be-better-safer/
35. Leslie Topp (2007), “The Modern Mental Hospital in Late Nineteenth-Century Germany and Austria: Psychiatric Space and Images of Freedom and Control,” in Madness, Architecture and the Built Environment: Psychiatric Spaces in Historical Context, ed. Leslie Topp, James Moran and Jonathan Andrews (London and New York: Routledge), 244.
36. McLaughlan, “One Dose of Architecture, Taken Daily,” 35; Digby, Madness, Morality and Medicine.
37. Anon (1908), “Proposed New Hospital for Mental Diseases,” The Lancet 171, no. 4410: 728–9.
38. Anon, “Proposed New Hospital for Mental Diseases.”
39. McLaughlan, “One Dose of Architecture, Taken Daily.”
40. Samuel Tuke (1964), “Description of the Retreat (1813),” reprinted in Description of the Retreat With an Introduction by Richard Hunter and Ida Macalpine (London: Dawsons of Paul Mall); Scull, Museums of Madness; Digby, Madness, Morality and Medicine; Smith, Cure, Comfort and Safe Custody.
41. World Health Organization (1953), The Community Mental Hospital. Also refer to T.F Main (1946), “The Hospital as a Therapeutic Institution”, Bulletin of the Menninger Clinic 10, no. 3: 66–71; David Clark (1965), “The Therapeutic Community Concept, Practice and Future,” The Journal of Mental Science 111: 947–54.
42. Jolanda Maas et al. (2009), “Social Contacts as a Possible Mechanism behind the Relation between Green Space and Health,” Health & Place 15, no. 2: 586–95; Gayle Souter-Brown (2015), Landscape and Urban Design for Health and Well-Being: Using Healing, Sensory and Therapeutic Gardens (Oxon & New York: Routledge); Ulrich et al., “A Review of the Research Literature,” 61–125.
43. Leon Festinger et al. (1950), Social Pressures in Informal Groups: A Study of Human Factors in Housing, vol. 11 (New York: Harper Bros); David Halpern (1995), Mental Health and the Built Environment: More than Bricks and Mortar? (London: Taylor and Francis); A. Baum and G.E. Davis (1980), “Reducing the Stress of High-Density Living: An Architectural Intervention,” Journal of Personality and Social Psychology 38, no. 3: 471–81; I. Altman and M.M. Chemers (1984), Culture and Environment (Monterey, CA: Brooks & Cole Publishing); Gary W Evans (2003), “The Built Environment and Mental Health,” Journal of Urban Health: Bulletin of the New York Academy of Medicine 80 no. 4: 536–55; Ulrich et al., “Psychiatric Ward Design Can Reduce Aggressive Behavior,” 53–66.
44. Stence Guldager cited in Troldtekt, “Innovative Architecture is Good for Mental Health,” https://www.troldtekt.com/News/Themes/Healing_architecture/Innovative_architecture_is_good_for_mental_health (accessed June 30, 2019); Clare Hickman and “Cheerful Prospects (2009).
45. Frank Pitts cited in Patricia Wen (2012), “For Mentally Ill, A Design Departure,” B News, August 16, https://www.boston.com/news/local-news/2012/08/16/for-mentally-ill-a-design-departure
46. Ellenzweig with Architecture Plus, “Massachusetts Department of Mental Health, Worcester Recovery Center and Hospital – Worcester, MA,” Healthcare Design (2013), July 30, https://www.healthcaredesignmagazine.com/architecture/massachusetts-department-mental-health-worcester-recovery-center-and-hospital-worcester-ma/
47. Sane Australia (2003), “A Life Without Stigma,” July 25, http://apo.org.au/resource/life-without-stigma; Otto F Wahl (2012), “Stigma as a Barrier to Recovery from Mental Illness,” Trends in Cognitive Sciences 16, no. 1: 9–10; New Zealand Ministry of Health and Health Promotion Agency (2014), “Like Minds, Like Mine National Plan 2014–2019: Programme to Increase Social Inclusion and Reduce Stigma and Discrimination for People with Experience of Mental Illness,” May 20, https://www.likeminds.org.nz/assets/National-Plans/like-minds-like-mine-national-plan-2014-2019-may14.pdf; G Moon (2000), “Risk and Protection: The Discourse of Confinement in Contemporary Mental Health Policy," Health & Place 6, no. 3: 245; R. Allen and R.G. Nairn (1997), “Media Depictions of Mental Illness: An Analysis of the Use of Dangerousness,” Australian & New Zealand Journal of Psychiatry 31, no. 3: 375–81; Greg Philo et al. (1994), “The Impact of the Mass Media on Public Images of Mental Illness: Media Content and Audience Belief,” Health Education Journal 53, no. 3: 271–81.
48. G Moon (2000), “Risk and Protection,” 239–50; T.F Main (1948), “Rehabilitation and the Individual,” in Modern Trends in Psychological Medicine, ed. Noel Haris (London: Buttefwork & Co. Ltd); D.A Fuller, E. Sinclair, and J. Snook (2016), “Released, Relapsed, Rehospitalized: Length of Stay and Readmission Rates in State Hospitals: A Comparative State Survey,” 2016, https://www.treatmentadvocacycenter.org/storage/documents/released-relapsed-rehospitalized.pdf ; Leila Salem et al. (2015), “Supportive Housing and Forensic Patient Outcomes,” Law and Human Behavior 39, no. 3: 311.
49. National Institute for Health and Clinical Excellence, Manchester (2016), “Transition between Inpatient Mental Health Settings and Community or Care Home Settings: Guideline,” August, https://www.nice.org.uk/guidance/ng53/evidence/full-guideline-pdf-2606951917
50. Catherine Clark Ahern et al. (2016), “A Recovery-Oriented Care Approach,” 47.
Bibliography
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors The research methodology was conceptualised by RM and CL. Data collection was completed by RM, CL and DJ. Analysis was completed by RM and CL, in accordance with the conceptual model developed by RM for her doctoral thesis (2014). Figures/diagrams were created by RM. The manuscript was prepared by RM.
Funding This study was funded by the Victorian Health and Human Services Building Authority (commissioned study).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.